A radical shift in the provision of healthcare is occurring. Within the past decade, advances in medical technology, changes in reimbursement structures, the desires and complex care needs of an aging population, and innovative care delivery models have initiated a shift from providing care in hospitals to outpatient settings. And more recently, the acceleration and amplification of these factors is pushing healthcare options even further from the traditional inpatient and outpatient settings towards acute and subacute care in the home. There are advantages and challenges to providing care in the home. It can be cost-effective and convenient, reducing unnecessary hospital admissions and giving patients the opportunity to receive the care they need where they are most comfortable. But as a newer model of care, there is not a well-established base of knowledge for undertaking this type of service or for supporting it through the built residential environment.
The evidence base for design that supports the provision of healthcare at home falls into two general categories:
Research literature and
Expert knowledge (e.g., publications from regulatory groups, experience-based opinions from key industry experts).
While this paper aims to present the salient research on design strategies that specifically facilitate healthcare at home, this is an emerging area; and while there may be an abundance of general strategies for consideration, there is little empirically supported evidence. Because Aging in Place and Universal Design approaches are highly relevant to the provision of healthcare at home, this paper draws largely from evidence in these two areas. These evidence-based design strategies contribute to physical and psychosocial needs of both patients and care providers. The findings include considerations for:
Building and room layout (configuration);
Patient-handling equipment;
Furniture;
Accessibility fixtures;
Storage;
Waste disposal;
Flooring;
Lighting;
Technology; and
Home aesthetics.
The concepts and solutions included in this paper may be most useful to owners, designers, and healthcare institutions on an as-needed basis in relation to remodeling, retrofitting, and adding to existing homes to support healthcare services. However, as Healthcare at Home is becoming more commonplace as a practice and a term, there is an opportunity to shift thinking in typical residential design towards a more sustainable concept of home – how home can support health and healing.
Background
Older adults with acute and chronic conditions who are stable enough to be treated at home are the primary audience for this rapidly growing healthcare industry (Bureau of Labor Statistics, 2018). However, the span of the home healthcare net is expanding to capture many other groups, including patients in rural areas, patients in rehabilitation, and patients of all ages with chronic illness (Cryer, Shannon, Van Amsterdam, & Leff, 2012; Leff et al., 2005).
TERMS FOR AND TYPES OF
HEALTHCARE AT HOME (Caplan et al., 2012)
Hospital in the Home (HITH)
Hospital at Home
Home Healthcare
Home Hospitalization
Early Supported Discharge
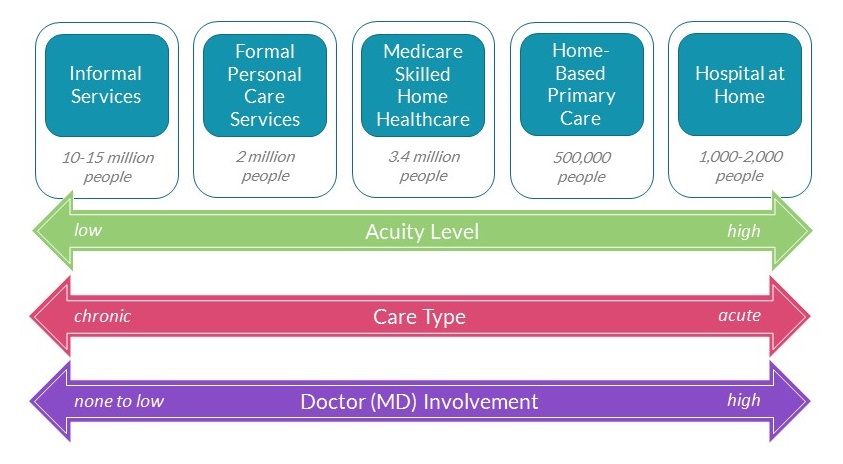
Healthcare at Home services span a range of care needs (Figure 1), including low- to high-acuity levels and chronic to acute care (Weisfeld & Lustig, 2015). Complex care, such as dialysis, chemotherapy, and intravenous (IV) administration of antibiotics and other home infusion therapies, vitamin injections, and diabetes management all can be supported in the home by advances in technology (National Research Council, 2011). Rehabilitation for acute conditions is also increasingly common in the home setting (Marcheschi, von Koch, Pessah‐Rasmussen, & Elf, 2018). Additionally, there is a range of provider types, from informal services provided by family and/or home care aides, to more formal skilled care, to models where the involvement of a medical doctor (MD) is substantial.
Figure 1. Spectrum of Services and Supports for Healthcare at Home. Source: Bruce Leff and Elizabeth Madigan (2014).
While various forms of Healthcare at Home have existed for some time, the trend towards more hospital-level acute and subacute care is relatively recent. Historically, agencies that deliver home healthcare have built their programming around Medicare insurance structures, but new models related to the Patient Protection and the Affordable Care Act (ACA), including accountable care organizations (ACOs) and bundle payment arrangement have reset the paradigm. These emerging models incentivize provider organizations to operate differently, from the software systems they use to the delivery of care (Weisfeld & Lustig, 2015). New models of acute care in the home are growing all around the country, and organizations like the Institute for Healthcare Improvement (IHI) are engaging in efforts to evaluate and test these initiatives (Wardlow, 2018).
Additionally, recent legislation passed through the Centers for Medicaid and Medicare Services (CMS) may make home renovations that support Healthcare at Home more feasible. Beginning in 2019, individuals enrolled in Medicare Advantage Plus (about one-third of those insured by Medicare) may be eligible for several new health-related benefits, including home aides to help with activities of daily living, palliative care at home, home safety devices, and home modifications, such as grab bars and wheelchair ramps (Span, 2018). While some private insurers that underwrite Advantage plans have been offering these incentives for years, this new legislation means that home modification opportunities will be more accessible for more Medicare recipients across the board.
ADVANTAGES OF HEALTHCARE AT HOME
A 19% decrease in mortality; better functional outcomes for patients; better receipt of medication (Caplan et al., 2012)
Shorter stays, fewer procedures, less delirium, greater satisfaction, similar functional outcomes (Leff et al., 2005)
Monetary savings for home hospice when compared to standard inpatient palliative care (Brumley et al., 2007)
Dollar-for-dollar reduction in medical expenses related to serious falls (Eriksen et al., 2015)
Home-based patients were more physically active, with a trend toward more sleep (Levine et al., 2018).
Healthcare at Home: Advantages
Healthcare services provided in the home can be beneficial for healthcare organizations and patients alike. For many patients, healthcare at home is more comfortable and convenient than a hospital stay. In addition to the facilitation of independence, Home Healthcare can reduce unnecessary hospitalization and associated risk of known complications, including healthcare-associated infections (Covinsky et al., 2003; Leff et al., 2005).
Studies have found Healthcare at Home may be more cost-effective than providing that same care in a traditional medical setting (Caplan et al., 2012; Cryer et al., 2012; Levine et al., 2018). In fact, one study that tested a model developed by Johns Hopkins found that when made available to Medicaid patients, costs were 19% lower compared to those for similar inpatients (Cryer et al., 2012). Additionally, the average “length of stay” (time patients received home-based care services) was shorter than length of stay for hospitalized patients (3.2 vs. 4.11 days), and yet these home care patients actually had more face-to-face time with clinicians (Cryer et al., 2012). Another study found that average cost of care for home patients was 52% lower than in-hospital care, and the average cost for the acute care plus 30-day post-discharge period for home patients was 67% lower, with fewer readmissions (Levine et al., 2018).
Home environments may decrease some of the burden on an over-saturated healthcare system (including emergency departments and hospitals with limited bed capacity), especially as the aging population continues to grow at a rapid rate (Cohn & Taylor, 2010). Healthcare at Home can be a convenient option for patients who face challenges getting to a clinic (e.g., transportation, accessibility, availability), or simply prefer not to go (Simmons-Duffin, 2018). Homes that support healthcare services for eligible recipients may also reduce the necessity to move into permanent assisted living, long-term care, and skilled nursing facilities.
Healthcare at Home: Challenges
While there are numerous advantages to Healthcare at Home, there also are many challenges. The home healthcare industry is growing rapidly, but there are still only a few healthcare organizations that offer formal home-care models for primary and hospital-level care. Johns Hopkins (Maryland) has developed the most well-known and established model, which has been adopted by several institutions across the United States since its inception in 1995(Johns Hopkins Hospital at Home, 2015). Other examples include Ohio Veterans Administration Hospital in Home program and Presbyterian Healthcare Services of New Mexico’s Hospital at Home program. Until this type of program becomes more common, the research on patient-centered health outcomes when compared to inpatient care (full or partial substitution) is also likely to be limited.
There are numerous challenges related to technological capabilities in the home environment. For instance, electronic medical records (EMRs) are not always available to home healthcare agencies, and home-based internet may not support access to the ones that do exist(Parker et al., 2018; Weisfeld & Lustig, 2015). Many Healthcare at Home models benefit from remote monitoring (e.g., video, automated calls, etc.) made possible by telehealth applications. Reimbursement for telehealth through Medicare is currently limited to specific circumstances, and is often too low to be attractive to providers(Center for Connected Health Policy, 2016), making it difficult to implement at a large scale (Weisfeld & Lustig, 2015). However, telehealth reimbursement models are evolving. In February 2018, the “Creating High-Quality Results and Outcomes Necessary to Improve Chronic Care” (CHRONIC) Act of 2017 was approved by the federal government. Beginning in 2020, the law will allow ACOs to reimburse telehealth for Medicare beneficiaries suffering from chronic illness Becker & Spitzer, 2018). However, the complexity of billing for “specialty” telehealth services will likely take several years for insurers to support as the norm.
Even when home healthcare programs are available, home modifications to support safe delivery of care may be cost prohibitive. Residential design tends to be oriented towards young, healthy, able-bodied adults and does not usually support accessibility needs, much less healthcare services. The cost and degree of modifications needed to support the provision of care is largely dependent on the level of care needed as well as the age, type, and condition of the home. For instance, simple modifications such as the installation of grab bars, railings, and ramps do not require extensive renovations and are likely to be much less expensive for a homeowner when compared to the cost of a visit to the emergency department or a hospital stay after a fall (Eriksen, Greenhalgh-Stanley, & Engelhardt, 2015). However, the grab bar (often seen as a sort of panacea for mobility-impaired persons), can only go so far in supporting Healthcare at Home. While Medicare is likely to cover the cost of grab bars, many questions remain: Will the cost of structural provisions and labor to install the grab bars be covered? What happens when unforeseen renovation costs arise during installation? Will more expensive grab bars that are designed to look like towel bars be covered or subsidized? If not, how might the appearance of basic metal grab bars affect the homelike aesthetic, and consequently, the resale value of the home? Further, the cost for more extensive renovations or complete remodels, additions, or new builds to accommodate larger equipment and structural changes (e.g., structural provisions for ceiling-mounted lifts) can be substantial.
I was recently asked. . . to place a midline in somebody’s arm and the situation was just horrific; the living situation of the patient. Very cluttery, no place [available], we didn’t have one, not even a table to use (Markkanen et al., 2007, p. 327).
Another challenge for Healthcare at Home arises for patients who do not own their home. The potential cost savings of accommodating healthcare delivery in the home does not always translate to patients living in rental properties. Property owners may not allow for home modifications, or if they do, modifications may not be feasible due to the size, layout, location, or age of the residence. Hospital-level care in the home can be especially challenging in urban areas where small apartments and high-rise buildings can make it difficult to bring in necessary healthcare equipment.
Another challenge facing home healthcare is the difficulty in measurement and evaluation of outcomes. Studies focused on patient experience and preference often rely on self-report measures, which are not always reliable. Patient conditions, circumstances, and home environments vary widely (e.g., size, type, condition, geographic area).
Because of the variety of home environments, design solutions to support safe delivery of care cannot be easily standardized (Kim, Geiger-Brown, Trinkoff, & Muntaner, 2010).
There is also little ability to control the conditions and occupational safety in the home as a workplace for care providers. A systematic review conducted by Hignett et al. (2016) provides a comprehensive overview of the issues. There are a range of providers in the home healthcare arena, from doctors to nurses and aides, and in many cases homecare workers are organized by informal, non-governed agencies where oversight is sometimes lacking (Kim et al., 2010). Home care providers are frequently working alone and face immense risk of harm. Studies have found the following examples of hazards care providers face in the home:
Musculoskeletal injuries from patient handling, slips/trips/lift injuries from dangerous flooring/rugs/stairs (Polivka et al., 2015),
Sharps injuries (Markkanen et al., 2007; Quinn et al., 2009),
Exposure to biohazards in unsanitary environments (Markkanen et al., 2007; Polivka et al., 2015),
Pests – mice and rats, insects, etc. (Polivka et al., 2015),
Assault injuries from patients (Galinsky et al., 2010), and
Mental health stressors (Markkanen et al., 2007).
The Evidence Base
There is limited research available on the role of the built environment in safe and effective delivery of healthcare in the home, for both patients and providers. The evidence that does exist is largely rooted in Universal Design and Aging in Place approaches. Additionally, there is some evidence on the topic of accessibility, a common thread in the research among all three design approaches. For the purposes of this paper, the term “accessibility” refers to the concept of design to support the ability to access and use the physical environment. This includes but is not limited to Americans with Disabilities Act (ADA) accessibility regulations. Before exploring the evidence base, it may be helpful to consider the relationship among the three design approaches.
Healthcare at Home and Aging in Place are terms that denote differences in a person’s abilities and needs as well as corresponding adaptations to the environment. Abilities evolve and shift throughout the life course, both on a temporary and permanent basis, and each of these design approaches can be applied to support the health, well-being, and recovery of an individual in their home. Figure 2 shows the typical application for these approaches in the context of life course and ability. Achieving alignment between abilities, needs, and environment – without having to change the environment as abilities and needs change – is the underlying philosophy of the Universal Design approach. Ideally, a home that is universally designed would support Aging in Place and Healthcare at Home. Similarly, a home that is designed for Aging in Place should support Healthcare at Home. Sadly, this is not always the case.
Figure 2. Residential Design Approaches in the Context of Biopsychosocial Abilities across the Life Course
Ramps that enable accessibility and mobility into and out of the home are an example of a design consideration that bridges the three approaches. Ramps benefit individuals of all ages receiving healthcare services at home, provide temporary assistance to individuals using a wheelchair or on crutches for rehabilitation, and provide permanent assistance to individuals who wish to age in place. Ramps could also be considered a Universal Design feature, as they benefit others living in the home at every age and every different level of ability or need (consider the toddler learning to walk, a new parent pushing a stroller, or anyone carrying unwieldy groceries, gifts, or furniture).
Figure 3. Concept vs. Reality: Alignment among Design for Healthcare at Home, Aging in Place, and Universal Design
Like any design concept (and, perhaps, more than most), exceptions to the rule and the differences between the ideal and reality abound (Figure 3). Design for Aging in Place as a concept is meant to support the needs of all individuals as they age so they can stay in the same place, and would ideally be inclusive of the needs of any person requiring Healthcare at Home. The reality is that designs that are called “Aging in Place” tend to be tailored to the abilities and needs of frail older adults. Likewise, when we see real-world examples of Healthcare at Home, the environment tends to be specialized for one person’s specific health condition, and would need to be adjusted to meet another individual’s specific healthcare needs.
Using an evidence-based design process requires drawing from these related topics and extracting the most pertinent information. This paper includes evidence-based design considerations drawn from Aging in Place, Universal Design, and Accessibility approaches where relevant to design that supports the specific circumstances of Healthcare at Home. It is worth noting that most of the design strategies have not undergone empirical testing.
Design for Healthcare at Home
The research on design for Healthcare at Home spans a variety of different perspectives, including the various patient populations (i.e., the people), the range of equipment/technology, the caregiving and daily living activities (i.e., tasks), and the physical environment. Beer, McBride, Mitzner, & Rogers (2014) use a human-systems perspective (Figure 4), which considers the dynamic relationship among all or several of these factors at once. As in any application of evidence-based design, a systems view must be considered. The physical environment (including the home, equipment, furniture, etc.) can support and facilitate safety, comfort, and healing, but the people and tasks (e.g., protocol, processes, and human behavior) must be considered simultaneously to address the abilities and limitations of users in order to enhance opportunities for positive outcomes.
Figure 4. Systems View of Healthcare at Home. Adapted from Beer et al. (2014).
Generally, the research on design for Healthcare at Home points to numerous challenges for both providers and patients in the home healthcare setting, and a few design strategies that aim to address two main outcome areas: physical needs and psychosocial needs.
Physical Needs
How can the design of an environment make life easier and safer for people receiving and providing healthcare in the home? A review of the research literature and expert knowledge on design for Healthcare at Home to support physical needs reveals that the most salient themes are accessibility and physical safety for activities of daily living. Evidence-based design strategies and interventions that support physical safety include the following:
Building and room layout (configuration),
Patient-handling equipment,
Furniture,
Accessibility fixtures,
Storage,
Waste disposal,
Flooring,
Lighting,
Technology, and
Home aesthetics.
Building and Room Layout (Configuration)
INTERVENTIONS THAT SUPPORT PHYSICAL SAFETY
Layout (configuration)
Patient-handling equipment
Furniture
Accessibility fixtures
Storage
Waste disposal
Flooring
Lighting
Technology
Home aesthetics
The layout of a home environment can have important implications for delivering care safely, supporting activities of daily living, and minimizing risk of injury, especially for impaired, elderly, or otherwise physically compromised individuals. The location of care delivery in the home depends on the level of care needed; for instance, the bedroom may be more appropriate for acute care, while the living room or kitchen may support care for chronic conditions and primary care procedures such as blood pressure checks and medication delivery.
Planning for a renovation or remodel to support home healthcare needs can be challenging when future needs are unknown. Patients and designers may want to start by considering how the home might accommodate some of the more challenging healthcare needs that may arise, and prioritize from there to determine what is most critical and feasible. Common considerations related to the general layout include space for ramps/stair lifts, patient mobility and handling devices, and medical equipment. In addition to the space for the equipment itself, it is necessary to include appropriate clearances (e.g., for turns, hallway-widths, around furniture) that support safe navigation around the home (AARP, 2016; Beer et al., 2014; National Association of Home Builders, 2016). Most Healthcare at Home experts agree that when possible, care areas, which generally consist of a bedroom and three-fixture bathroom, benefit from being located adjacent to one another on the main level (street level) of the home (AARP, 2016; Mitka, 2001; National Association of Home Builders, 2016).
Two studies (Leiss, 2012; Markkanen et al., 2007) specifically mention the importance of privacy, acoustics, and minimizing stimulation. Designated spaces for care that are quiet or can be closed off (at least temporarily) from distractions from pets and children are also helpful. This is especially important to support safe care procedures, such as medication preparation, use of sharps, exams and treatment, as well as charting (Beer et al., 2014; Exley & Allen, 2007; Markkanen et al., 2007). A quiet designated “clinical” area can facilitate better communication between patients and care providers, as well as communication with remote providers through telesupport systems (Beer et al., 2014). Care providers may also benefit from access to a designated, quiet, separate area for focused work such as charting (Beer et al., 2014).
Patient-handling Equipment
Just like in the hospital, patient handling in the home poses the risk of musculoskeletal injury and/or falls, especially during transfer tasks, for both providers and patients (Beer et al., 2014). Patient-handling equipment, especially in common transfer areas (bedroom, bathroom, garage) can help to reduce these risks and includes lifts, braces, and physical support furniture (e.g., hospital beds, chair lifts) (Beer et al., 2014; Collins, Wolf, Bell, & Evanoff, 2004; Dellve, Lagerström, & Hagberg, 2003; Kim et al., 2010; Parsons, Galinsky, & Waters, 2006). A study by Collins, Wolf, Bell, and Evanoff (2004) found that when a “best practices” musculoskeletal injury prevention program that included mechanical lifts and repositioning aides was implemented in the home, as well as employee training on lift usage, there was a significant reduction in resident handling injury incidence, workers’ compensation costs, and lost workday injuries.
The expense for mechanical lifts and/or structural provisions to integrate ceiling-mounted lifts in the home can be substantial. Based on similar methods for expenditure decision making in healthcare, Douglas et al. (2014) have created a systematic methodology – an algorithm – to help determine the need for mechanical or stand lifts in the home. Safety for patients and caregivers is the primary consideration in this algorithm. This algorithm (Figure 5) may be applicable as a framework for determining the need for other types of equipment and renovation expenditures in the home setting to support healthcare as well, on the basis of patient and caregiver safety.
Figure 5. Framework for Healthcare at Home Equipment/Renovation/Remodel Decision-Making Algorithm. Adapted from Douglas et al., (2014) Algorithm for Safe Patient Transfer.
Furniture
When considering furniture to support healthcare in the home, physical safety is a priority. Transferring in and out of bed and chairs safely is an ongoing concern for patients who have compromised mobility, as well as for providers or family members providing assistance (Van Hoof & Kort, 2009). The level of support recommended for getting up and down from a seated or lying position may depend on the individual’s need for rehabilitation or rest. For some, too much support may hinder their rehabilitation.
For patients who need to avoid risk of strain, there are several features and settings available for supportive furnishings. Standard single beds or electric or hydraulic hospital beds with adequate clearance on both sides may be necessary, as the smaller size can facilitate safe, efficient care and transfers for both patients and providers (Taylor & Donnelly, 2006). Healthcare at Home experts recommend adjustable lounge chairs with elevated footrests, or sit-to-stand chairs, or lift chairs containing built-in lift mechanisms (Cox & Cox, 2000; Marcheschi et al., 2018; Parsons et al., 2006).
Visibility is key for patients when navigating around objects or trying to get in and out of furniture. High contrast and color differentiation between furniture and surroundings can improve visibility of objects for patients, especially for those with visual impairment (Van Hoof & Kort, 2009). Adequate lighting of furniture is also essential for safe navigation (see “Lighting” below).
Accessibility Fixtures
When a person is suffering from a health condition that affects their mobility, simple daily activities and use of everyday fixtures around the home can become extremely challenging. The difference between stairs or ramps at the entrance of the home can dictate if care at home is even an option. The location, height, and type of switch, rail, handle, or plumbing fixture can greatly frustrate or enable someone who is temporarily or permanently mobility impaired (Brookfield et al., 2015).
Handrails, grab bars, and ramps that facilitate mobility and accessibility are essential for a patient’s ability to safely navigate activities of daily living, engage in treatment and rehabilitation activities, and enter and exit their home. A study by Brookfield et al. (2015) found that for stroke survivors, the presence or absence of handrails in the home was, respectively, either a facilitator or barrier for mobility and participation in activities.
Storage
Adequate, easily accessible storage can address a variety of physical safety challenges in a home healthcare setting. Much of the research that mentions the importance of storage has to do with reducing the risk of falls and/or physical strain when accessing medical supplies: equipment and devices, medications, sharps, and frequently used items. Options for locked or high, out-of-reach storage may help to keep medications and/or medical equipment away from children or patients who need assistance in ensuring their correct dosage (for example, individuals who have dementia) (Green, 2018).
Organizing personal protective equipment (PPE) in easily accessible storage may reduce risk of infection for care providers in the home, (Green-McKenzie, Gershon, & Karkashian, 2001). A study by Leiss (2012) found that extreme clutter contributed to the risk of blood exposure rates among home care and hospice nurses. Nurses reported having to clear a space around the patient to set up medical supplies (Leiss, 2012). Home healthcare patients and providers benefit from adequate storage options so that care providers are able to easily access or clear a clean workspace for safe delivery of care (Beer et al., 2014).
A designated, accessible storage location for instructional materials can help care providers with proper use of medical equipment, lift technology, and other devices (National Research Council, 2011). Instructional materials are the instructions provided by manufacturers of medical equipment, technology, devices, and medications, as well as proper procedures for certain tasks. Storage should be located as close to the equipment as possible. A study by Beer et al. (2014) found that providers are often faced with unexpected complications that arise with medical devices and would benefit from step-by-step instructions for dealing with these scenarios.
Waste Disposal
One of the more well-researched topics in the area of the home healthcare environment and safety is focused on the risks providers face related to improper waste disposal, most commonly related to punctures or cuts from medical devices with sharp points or edges, commonly referred to as “sharps.” Many home care procedures require use of sharps, and healthcare personnel are at risk for blood infections if they are stuck or cut by sharps used by patients (Brouillette et al., 2017; Leiss, 2012; Quinn et al., 2009). A study by Quinn et al. (2009) found that contact with waste was a top risk factor for exposure among aides and nurses. Storage that is easily accessible and adequately sized for sharps disposal may help to reduce exposure (Markkanen et al., 2007).
Individuals receiving healthcare at home may have toileting needs and/or injuries that create a plethora of safety issues related to waste and cleanup of body fluids. Home care workers frequently are exposed to blood and other body fluids and need to be able to quickly access waste disposal and cleaning equipment when these events occur. A study by Quinn et al. (2009) across nine home health care agencies and two labor unions in the northeast U.S. found that 15.1% of nurses and 6.7% of aides experienced blood and body fluid exposures during their home health care career. The authors of this study mention that the estimates for blood and body fluid exposures are likely low because the nurses and aides reported that these types of exposures are “part of our job” and occur “all the time” (Quinn et al., 2009).
Flooring
Similar to research findings in the area of healthcare facility design, numerous intrinsic (inherent to the patient) and extrinsic factors (external to the patient) contribute to falls in the home environment. Just like a fall in the hospital, falls at home are costly, and a fall for a patient receiving healthcare at home can have a negative impact on their recovery process and even sometimes result in death. According to a report by the U.S. Department of Housing and Urban Development, “by 2020, expenditures related to injuries sustained as a result of falls by seniors are projected to cost nearly $59.7 billion. Approximately one-third of adults age 65 years or older fall each year; the majority of these falls occur in the home” (Healthy Housing Solutions, 2017).
The majority of research on falls in the home focuses on education and programs targeted towards fall prevention, through physical activities related to exercise and balance (Healthy Housing Solutions, 2017). Few studies look specifically at the role of the physical home environment on fall reduction. The research that does exist in this area shows a link between hazards such as dangerous flooring/floor coverings/stairs and an increase in the risk of slips, trips, and falls for both patients and care providers in the home (Clemson, Cumming, & Roland, 1996; Polivka et al., 2015). A recent cluster randomized control trial included a combination of interventions including handrails, minor repairs, and visibility and slip-resistant edging for outside steps; handrails for internal stairs; grab rails for bathrooms and toilets; adequate outside lighting; secured edges of carpets and mats; non-slip bathmats; and slip-resistant surfacing for outside surfaces such as decks (Keall et al., 2015). According to the authors, a statistically significant reduction of 26% in the falls injury rate was found when comparing the control homes to the intervention homes.
However, a systematic review conducted by Lord, Hylton, and Sherrington (2006) concluded that, while reducing environmental hazards in the home may be useful for older adults with a history of falls and mobility limitations, the strategy may not be equally effective for those with low risk of falls. This study highlights the importance of a systems view including both the physical environment as well as strategies to address the activities, capabilities, and limitations of the individual in reducing the risk of falls. A more recent randomized controlled trial conducted by Cumming et al. (2015) supports this point. While home modifications may reduce falls, the effect appears to be dependent on the patient receiving training from occupational therapists to address their individual characteristics and related activities in the home.
A study by Polivka et al. (2015) found that care providers reported trip and slip hazards in the kitchen more frequently than other rooms in the home, followed closely by the bathroom. Participants mentioned obstacles on the kitchen floor such as rugs, water or grease spills, clutter, and damaged flooring when discussing hazards they faced when providing care (Polivka et al., 2015). Slip-resistant flooring materials that hold up to wear and tear, avoiding the use of rugs and other coverings, and appropriate mobility aids can help patients and care providers safely navigate the kitchen and bathroom (Green, 2018).
Perritt, McCune, and McCune (2005) examined the impact of carpet texture and pattern on walking time and stability on persons with Alzheimer’s disease. They found that patterns with the lowest contrast and smallest motifs were associated with significantly shorter walk time and fewer incidents (e.g., stumbling, side-stepping, veering, falling, etc.). Experts tend to agree that flooring with high-contrast patterns is a risk factor for falls and should be avoided (Calkins, Biddle, & Biesan, 2012). Alternating ”hot spots” and shadows created by lighting can also be a concern, regardless of flooring pattern (McMurdo & Gaskell, 1991).
Lighting
Just as in healthcare facility design, good lighting can support several important outcomes in the home healthcare setting. Adequate lighting is essential for aging populations, as the changes that occur in the eye with aging make it difficult to absorb light, especially in the blue range, and difficult to adjust to changes in brightness or glare. Strategic lighting solutions can reduce the risk of falls for patients of all ages who are physical or mentally compromised by their conditions and/or medications as they navigate around their home. This is especially problematic at night when patients are most likely to try to get out of bed and go to the bathroom or kitchen unassisted (Van Hoof & Kort, 2009). Amber or red colored light is beneficial to use during sleeping hours, as it does not cause the pupils to dilate. Smart home sensor technology can utilize amber-colored lights to illuminate the path from the bed to the toilet, including rope lighting placed vertically around doorways and furnishings, and horizontally under beds and kick plates to provide visual cues and keep patients oriented (Davis, Wilkerson, Samla, & Bisbee, 2016; Figueiro, Gras, et al., 2008; Figueiro, Saldo, et al., 2008; “Meridian at Home,” 2017; N2Care LLC, 2017; National Research Council, 2011).
Circadian lighting interventions may prove beneficial in the home healthcare setting. A study by Figueiro et al. (2015) examined the effect of a lighting intervention in the home for people with dementia and their caregivers. The lighting intervention was designed to increase circadian stimulation during the day with light sources that have high short-wavelength content and high light output, similar to outdoor sun exposure. They found that the lighting increased circadian entrainment (the alignment of the internal biological clock rhythm with external cues from the environment) and sleep efficiency, and reduced symptoms of depression for participants with Alzheimer’s disease and related dementia. It is also worth noting that caregivers also benefitted from the lighting intervention; they also showed an increase in circadian entrainment, a seasonal effect of greater sleep efficiency, and longer sleep duration (Figueiro et al., 2015).
While the Figueiro study examined the effect of lighting levels on people with dementia, a study by Hopkins et al. (2017) looked at the effect on the general population of older people not diagnosed with dementia. In this study (which was conducted in care facilities, not the home), researchers found that blue-enriched lights increased daytime activity and reduced subjective anxiety. However, there were numerous drawbacks, including increased actual wake time (following sleep onset) and activity during sleep, and decreased actual sleep time, sleep percentage, and sleep efficiency. Subjective sleep quality also suffered. When considering circadian lighting options, it is important to keep in mind that the timing of exposure to different color wavelengths of lighting and different lighting in general affects different people in different ways.
Adequate lighting is essential in areas where providers perform exams and care procedures and need to be able to visually detect subtle changes, such as the hue of a patient’s skin. Moveable and adjustable exam lighting can help to support care procedures and facilitate visibility for telemedicine procedures (Hume & Looney, 2016).
Lighting can support infection control and medication safety as well. A study by Leiss (2012) found poor lighting to be one of the factors that contributed to risk of blood exposure during care procedures. Good lighting is necessary for safe medication dispensing by either providers or patients – when reading labels on medicine bottles and dosing medication (Mitka, 2001).
Technology
Advances in technology are a major reason that home healthcare is possible today, and there are numerous ways in which technology can help to support safety for both patients and providers. The advent of the “smart home” may support Healthcare at Home (or “Health Smart Homes”) through communication technology and ambient intelligent technology such as wearable sensors (Mshali, Lemlouma, Moloney, & Magoni, 2018). Telemedicine exam equipment (e.g., a laptop with integrated medical devices) can allow the in-home provider and/or patient to share information with remote care providers in real time (Hume & Looney, 2016). Design strategies to support this technology include adequate space for various technology set-ups near power, data, and conduit pathways for wired internet connections, or wireless access.
Like other design considerations in this paper, many technologies that support Healthcare at Home were originally derived to support Aging in Place. Aging Service Technologies (ASTs) have been developed in the hope of helping people live independently at home for as long as possible, with the potential to provide safety, security, and enjoyment as needs change due to aging. This type of technology may be beneficial for anyone receiving healthcare at home regardless of age, especially when dealing with cognitive and physical impairments. ASTs include sensor-based networks, fall- and wandering-detection technologies, and an array of electronic health applications (Lee & Xie, 2018).
Psychosocial Needs
While physical safety and physical health outcomes are usually the primary considerations when determining the prospect of healthcare in the home, the psychosocial needs of the patient and their family must be taken into account as well. The shift from resident to patient in one’s own home means a major shift in very personal, intimate, and private ways they experience “home” (Tanner, Tilse, & de Jonge, 2008). While home care can offer many benefits to one’s mental state, the same care may also present emotional challenges and disruption in the way a home feels thereafter.
INTERVENTIONS TO SUPPORT PSYCHOSOCIAL NEEDS
Layout (configuration)
Furniture
Accessibility fixtures
Technology
Home aesthetics
The literature on psychosocial and emotional needs in the context of Healthcare at Home is even more limited than the research on physical needs. However, social, cognitive, personal, and behavioral factors are key when designing to support better outcomes for patients receiving and staff providing healthcare in the home. The available evidence-based design strategies focused on supporting psychosocial needs of both patients and providers can be organized in the following physical environment categories:
Building and room layout (configuration);
Furniture;
Accessibility fixtures;
Technology; and
Home aesthetics.
Building and Room Layout (Configuration)
Adequate space for family, visitors, and pets can help to facilitate social support for patients receiving healthcare at home. This space becomes especially important for critical care and end-of-life care when the number of visitors may increase. Patients benefit from being able to die in the comfort of their own home with loved ones nearby, but with enough space so as to move out of the way during urgent care procedures (Exley & Allen, 2007). Care providers may also benefit from access to a designated space for personal respite from patient, family, and visitors (Dellve et al., 2003).
Furniture
Furniture that is easy to move and adjust (e.g., furniture with modular elements) can accommodate changing needs for the variety of patient types receiving a variety of care in their home. Flexibility in use and layout of furniture can also support “visitability” for the range of care providers, family, and guests who may be coming in and out of the home (How Housing Matters original, 2016). As mentioned above in regards to physical safety and furniture, single beds are preferable to double beds to facilitate safe, efficient care and transfers (Taylor & Donnelly, 2006). However, when considering the patient’s psychological well-being, a double bed to accommodate a partner may be a higher priority.
Accessibility Fixtures
While features that facilitate accessibility in the home (e.g., grab bars, handrails, and height-adjustable counters) have clear implications for physical needs, these can also greatly improve the psychosocial experience of Healthcare at Home. A study by Brookfield et al. (2015) found that stroke survivors would avoid certain activities – activities that could have an impact on their health or recovery such as bathing – simply because of the perceived risk. Stress and anxiety related to the possibility of falling, especially in the shower or tub, can be mitigated by the presence of grab bars and handrails in the home (Brookfield et al., 2015).
The occupational therapist told me to ask the municipality for a hospital bed with guard rail… but I am not that disabled. I love my bed and do not want to sleep alone for the rest of my life (Brodersen and Lindegaard, 2014, p. 277).
At the same time, standard accessibility fixtures sometimes have a sterile appearance, not easily integrated into the home setting. Many people have negative association with grab bars in particular – that they are a sign of growing old and something “I don’t need yet.” Designers hope to address this issue by softening the appearance, even developing “high end” luxurious versions of these features, to be better suited for residential setting.
I’m not encouraged to have a shower . . . there’s always that fear there . . . I’m not going to risk it every day. – Stroke survivor (Brookfield et al., 2015, p. 626)
Technology
There is a major trend in recent years towards internet-based behavioral and mental health services, which allows patients to receive the care they need with clinical staff from the comfort of their home. This option is attractive to many individuals suffering from behavioral health issues, as frequently reoccurring appointments take excess time to attend in person. Further, some patients are leery of the stigma associated with seeking services, and fear being recognized at a facility or office providing behavioral and mental health services.
Tele-support systems may help to address some psychosocial needs by supporting better communication among patients, providers, family, and other support systems (Beer et al., 2014). Various smart home technologies that monitor and evaluate health conditions and monitor daily activities may help to support increased independence for patients receiving care at home. However, there are tradeoffs to consider, such as decreased privacy. Many of these technologies are designed to gather continuous data on a person’s behavioral, physiological, and environmental activities in order to customize appropriate services. Research on this type of continuous monitoring by Rogers and Fisk (2010) found that concerns about privacy were conditional for older adults, and that generally, although privacy is a concern, the benefit of being able to stay in one’s own home and maintain general independence may be worth the intrusion.
When people are unwell, they may need social support more than ever, but it can be an especially challenging time to remain connected to a support system. Social isolation is one of the leading risk factors in early mortality (Holt-Lunstad, Smith, & Layton, 2010), and can be especially detrimental when health is already compromised. Social technologies may provide a means for people receiving healthcare at home to stay engaged with friends, family, or other interests. According to a study by Czaja et al. (2018) that focused on older adults, software applications that provide easy access to resources and opportunities for engagement and communication may enhance social connectivity and reduce loneliness.
Technology may also be able to help support the psychosocial needs of care providers. Healthcare staff, especially in rural areas, can feel quite isolated and lack the collegial support that is beneficial to avoid burnout in a mentally and emotionally taxing profession. As telehealth is becoming more common in Healthcare at Home care models (Hume & Looney, 2016), a variety of options (e.g., telephone support groups, teleconferencing, telepresence systems) are becoming available to support provider training and clinical care services.
If this (monitoring system) would keep me independent longer, I wouldn’t mind as much (Rogers & Fisk, 2010, p. 650).
There are arguments for and against the benefits of smart home technologies for patients with certain conditions receiving healthcare at home. Technology can facilitate daily life and many healthcare needs in the home for patients – for instance, automated blinds and temperature control and emergency communication systems. However, these complex features can create stress for new users, and especially for those with cognitive impairments. There is some skepticism about the value of certain information and communication technologies, especially for older adults who may not trust it, cannot or do not want to pay for it, or do not understand how to use it. While there are a variety of complex technologies that are challenging for any user, some research shows that once older adults adopt a particular technology they tend to use it just as frequently as younger adults (O’Brien, Rogers, & Fisk, 2012). More research is needed to fully understand the potential of a wide variety of technologies to support better outcomes and be adopted by aging adults and people receiving healthcare in the home (Lee & Xie, 2018).
Orpwood, Bjørneby, Hagen, Mäki, Faulkner, & Topo (2004) created the design recommendations for technology for people with dementia, which are likely to be universally helpful for any user. Technology should:
Not require any learning,
Look familiar,
Allow users to retain control,
Require a minimum of user interaction, and
Provide reassurance to the user.
Home Aesthetics
Setting up a home to support healthcare needs often means reorganizing the domestic arrangement to accommodate a variety of equipment that has a very non-domestic institutional aesthetic. The sudden presence of hydraulic beds, commodes, hoists, and specialized equipment can alter the domestic aesthetic we all desire in our homes. A study by Angus et al. (2005) looking at the personal significance of home for care recipients concluded that even though patients indicated a strong preference for home care over institutional care, the institutional presence in their home was a difficult adjustment. The authors conclude that the “progressive entanglement of the logics of the home and those of the healthcare system produced an ambiguity of place for recipients” (p. 182) with the aesthetics of the healthcare equipment in constant contrast to the home. Adequate storage space, such as cabinets and closets large enough to store medical gear, can help to reduce clutter and maintain the feeling of home (Exley & Allen, 2007; Sine, 2015).
It may be necessary to have a centrally located white board/tackable surface panel that supports communication and coordination regarding home healthcare services, provider information, scheduling, reminders, instructions for certain medical scenarios, and the patient’s needs (Van Hoof & Kort, 2009). This board should be located in a highly visible, frequently used area of the home, such as the kitchen. While communication technology options may be appropriate for some patients, these systems can be confusing, especially when different service providers are coming in and out of the home using different EMR systems, and patients and family members and visitors are crossing paths trying to keep everything straight. A physical board on the wall may be most appropriate and aesthetically fitting for home care coordination.
The home setting and health services and supports will become so synonymous that they may not be called home care; rather, they will just be modern health care. – Steven Landers, Visiting Nurse Association Health Group (Weisfeld & Lustig, 2015, p. 17)
While healthcare in the home means making these necessary changes to support a safe environment for care, there should be a balance between provisions for the safety and preservation of the personal effects and person-centered experience that make healthcare at home such an attractive option for healing in the first place. A study by Axelrod et al. (2009) found that features in the home that held sentimental significance, such as ornaments and lifetime possessions, could facilitate emotional recovery for stroke survivors.
The majority of the literature refers to individuals receiving care at home as “patients;” however, the individuals receiving care may or may not see themselves as patients in their own home. This is an important distinction in the way care is provided and design conducted.
The majority of the literature refers to individuals receiving care at home as “patients;” however, the individuals receiving care may or may not see themselves as patients in their own home. This is an important distinction in the way care is provided and design conducted. As the need grows, architects, designers, and medical equipment manufacturers should consider other strategies to reduce the institutional aesthetic of Healthcare at Home.
Conclusion
Healthcare at Home offers potential advantages over traditional healthcare options for both healthcare organizations and patients, including:
Lower costs (Caplan et al., 2012; Cryer et al., 2012),
Reduced strain on saturated healthcare facilities (Cohn & Taylor, 2010),
Greater patient autonomy (Covinsky et al., 2003),
Reduced risk of healthcare-associated infections (Leff et al., 2005),
Reduced length of stay (Brumley et al., 2007; Cryer et al., 2012), and
More patient-centered care (Cryer et al., 2012).
However, if the home is not properly equipped, or if a formal home-care model for hospital-level care is not available, hospitalization or a move into a rehabilitation or long-term care setting may be the only viable option for people with increasing healthcare needs.
Take for example the patient lift. If an individual has mobility limitations, and requires long-term Healthcare at Home services and assistance getting in and out of bed, toileting, and bathing, it may make sense to remodel the home to install a ceiling-mounted patient lift. In general, lifts would not be a design consideration unless the user is receiving healthcare at home. But what could design do to meet the need of the Healthcare at Home patient, without being so specialized that the design would be unappealing (i.e., too institutional/sterile/hospital-like) for others in the home and future residents? How can members of the healthcare and long-term care industries partner with the residential sector to affect change in this market? How can every home support healthcare?
Evidence-based design for Healthcare at Home is emerging. While there may be overlap among Universal Design, Aging in Place, and Healthcare at Home — especially in terms of accessibility — there are numerous opportunities for new research in these areas.
Owners, architects, and designers in the healthcare, long-term care, and residential sectors may be the best qualified to undertake the challenge of design for Healthcare at Home. Residential and healthcare design may seem an unlikely marriage at first glance, but there is a significant and growing need to support this union. We must ask: What are the opportunities for owners, designers, researchers, and other stakeholders to move the residential healthcare industry forward? Housing stock is limited and quickly becoming unsuitable for many users with diverse needs, such as our growing aging population and individuals who will need healthcare at home. We must find ways to design for all changing needs in our homes. With the potential benefits of Healthcare at Home, this sector deserves more attention, especially in terms of policy, design, and research.
This white paper was created with funding from the Angelo Donghia Foundation.
References
AARP. (2016, February). Aging Friendly Home Renovations and Improvements. Retrieved February 8, 2017, from Livable Communities website: http://www.aarp.org/livable-communities/housing/info-2016/aging-friendly-renovation-improvements.html
Angus, J., Kontos, P., Dyck, I., McKeever, P., & Poland, B. (2005). The Personal Significance of Home: Habitus and the Experience of Receiving Long-Term Home Care. Sociology of Health & Illness, 27(2), 161–187. https://doi.org/10.1111/j.1467-9566.2005.00438.x
Axelrod, L., Smith, P., Fitzpatrick, G., Ricketts, I., Burridge, J., Mawson, S., & Rodden, T. (2009). The reality of homes fit for heroes: Design challenges for rehabilitation technology at home. Journal of Assistive Technologies, 3(2), 35–43. https://doi.org/10.1108/17549450200900014
Becker, S., & Spitzer, J. (2018, March 2). The growth of telehealth and virtual care — reimbursement and more — 8 thoughts and issues. Retrieved from Becker’s Hospital Review website: https://www.beckershospitalreview.com/telehealth/the-growth-of-telehealth-and-virtual-care-reimbursement-and-more-8-thoughts-and-issues.html
Beer, J. M., McBride, S. E., Mitzner, T. L., & Rogers, W. A. (2014). Understanding challenges in the front lines of home health care: A human-systems approach. Applied Ergonomics, 45(6), 1687–1699. https://doi.org/10.1016/j.apergo.2014.05.019
Brookfield, K., Fitzsimons, C., Scott, I., Mead, G., Starr, J., Thin, N., … Ward Thompson, C. (2015). The home as enabler of more active lifestyles among older people. Building Research & Information, 43(5), 616–630. https://doi.org/10.1080/09613218.2015.1045702
Brouillette, N. M., Quinn, M. M., Kriebel, D., Markkanen, P. K., Galligan, C. J., Sama, S. R., … Davis, L. (2017). Risk of Sharps Injuries Among Home Care Aides: Results of the Safe Home Care Survey. American Journal of Infection Control, 45(4), 377–383. https://doi.org/10.1016/j.ajic.2016.11.018
Brumley, R., Enguidanos, S., Jamison, P., Seitz, R., Morgenstern, N., Saito, S., … Gonzalez, J. (2007). Increased Satisfaction with Care and Lower Costs: Results of a Randomized Trial of In-Home Palliative Care. Journal of the American Geriatrics Society, 55(7), 993–1000. https://doi.org/10.1111/j.1532-5415.2007.01234.x
Bureau of Labor Statistics. (2018, January 30). Home Health Aides and Personal Care Aides [Government]. Retrieved from US Department of Labor website: https://www.bls.gov/ooh/healthcare/home-health-aides-and-personal-care-aides.htm
Calkins, M. P., Biddle, S., & Biesan, O. (2012). Contribution of the Designed Environment to Fall Risk in Hospitals (pp. 1–100) [Research]. Retrieved from The Center for Health Design website: https://www.healthdesign.org/chd/knowledge-repository/contribution-designed-environment-fall-risk-hospitals
Caplan, G. A., Sulaiman, N. S., Mangin, D. A., Ricauda, N. A., Wilson, A. D., & Barclay, L. (2012). A Meta-Analysis of “Hospital at Home.” Medical Journal of Australia, 197(9), 512–519. https://doi.org/10.5694/mja12.10480
Center for Connected Health Policy. (2016). Telehealth Reimbursement Fact Sheet. Retrieved from http://www.cchpca.org/sites/default/files/resources/Telehealth%20Reimbursement%20Fact%20Sheet%20FINAL_0.pdf?utm_source=Telehealth%2BEnthusiasts&%3butm_campaign=113173f851-Issue_in_Focus_MACRA_Final_Rule_Marginal10_24_16&%3butm_medium=email&%3butm_term=0_ae00b0e89a-113173f851-343530453
Clemson, L., Cumming, R. G., & Roland, M. (1996). Case-Control Study of Hazards in the Home and Risk of Falls and Hip Fractures. Age and Ageing, 25(2), 97–101.
Cohn, D., & Taylor, P. (2010, December 20). Baby Boomers Approach 65 – Glumly. Retrieved September 30, 2016, from Pew Research Center’s Social & Demographic Trends Project website: http://www.pewsocialtrends.org/2010/12/20/baby-boomers-approach-65-glumly/
Collins, J. W., Wolf, L., Bell, J., & Evanoff, B. (2004). An Evaluation of a “Best Practices” Musculoskeletal Injury Prevention Program in Nursing Homes. Injury Prevention, 10(4), 206–211. https://doi.org/10.1136/ip.2004.005595
Covinsky, K. E., Palmer, R. M., Fortinsky, R. H., Counsell, S. R., Stewart, A. L., Kresevic, D., … Landefeld, C. S. (2003). Loss of Independence in Activities of Daily Living in Older Adults Hospitalized with Medical Illnesses: Increased Vulnerability with Age. Journal of the American Geriatrics Society, 51(4), 451–458. https://doi.org/10.1046/j.1532-5415.2003.51152.x
Cox, H., & Cox, D. (2000). Hospitals without Walls: A Journey through the Health-Care System. International Journal of Nursing Practice, 6(2), 105–109. https://doi.org/10.1046/j.1440-172x.2000.00188.x
Cryer, L., Shannon, S. B., Van Amsterdam, M., & Leff, B. (2012). Costs For ‘Hospital At Home’ Patients Were 19 Percent Lower, With Equal Or Better Outcomes Compared To Similar Inpatients. Health Affairs, 31(6), 1237–1243. https://doi.org/10.1377/hlthaff.2011.1132
Cumming, R. G., Thomas, M., Szonyi, G., Salkeld, G., O’Neill, E., Westbury, C., & Frampton, G. (2015). Home Visits by an Occupational Therapist for Assessment and Modification of Environmental Hazards: A Randomized Trial of Falls Prevention. Journal of the American Geriatrics Society, 47(12), 1397–1402. https://doi.org/10.1111/j.1532-
5415.1999.tb01556.x
Czaja, S. J., Boot, W. R., Charness, N., Rogers, W. A., & Sharit, J. (2018). Improving Social Support for Older Adults Through Technology: Findings From the PRISM Randomized Controlled Trial. The Gerontologist, 58(3), 467–477. https://doi.org/10.1093/geront/gnw249
Davis, R. G., Wilkerson, A. M., Samla, C., & Bisbee, D. (2016). Tuning the light in senior care: Evaluating a trial LED lighting system at the ACC Care Center in Sacramento, CA (Prepared in Support of the DOE Solid -State Lighting Technology GATEWAY Program No. Contract DE-AC05-76RL01830). Retrieved from U.S. Department of Energy website: http://energy.gov/sites/prod/files/2016/09/f33/2016_gateway-acc.pdf
Dellve, L., Lagerström, M., & Hagberg, M. (2003). Work-System Risk Factors for Permanent Work Disability among Home-Care Workers: A Case-Control Study. International Archives of Occupational and Environmental Health, 76(3), 216–224.
Douglas, B., Fitzpatrick, D., Golub-Victor, A., & Lowe, S. M. (2014). Should My Patient Use a Mechanical Lift? Part 2: Algorithm and Case Application. Retrieved January 9, 2019, from Home Healthcare Nurse website: https://nursing.ceconnection.com/ovidfiles/00004045-201403000-00006.pdf
Eriksen, M. D., Greenhalgh-Stanley, N., & Engelhardt, G. V. (2015). Home Safety, Accessibility, and Elderly Health: Evidence from Falls. Journal of Urban Economics, 87, 14–24. https://doi.org/10.1016/j.jue.2015.02.003
Exley, C., & Allen, D. (2007). A critical examination of home care: End of life care as an illustrative case. Social Science & Medicine, 65(11), 2317–2327. https://doi.org/10.1016/j.socscimed.2007.07.006
Figueiro, M. G., Gras, L., Qi, R., Rizzo, P., Rea, M., & Rea, M. S. (2008). A novel night lighting system for postural control and stability in seniors. LIGHTING RESEARCH & TECHNOLOGY, 40(2), 111–126. Retrieved from edswsc.
Figueiro, M. G., Hunter, C. M., Higgins, P., Hornick, T., Jones, G. E., Plitnick, B., … Rea, M. S. (2015). Tailored Lighting Intervention for Persons with Dementia and Caregivers Living at Home. Sleep Health, 1(4), 322–330. https://doi.org/10.1016/j.sleh.2015.09.003
Figueiro, M. G., Saldo, E., Rea, M. S., Kubarek, K., Cunningham, C., & Rea, M. S. (2008). Developing architectural lighting designs to improve sleep in older adults. The Open Sleep Journal, (1), 40–51.
Galinsky, T., Feng, H. A., Streit, J., Brightwell, W., Pierson, K., Parsons, K., & Proctor, C. (2010). Risk Factors Associated with Patient Assaults of Home Healthcare Workers. Rehabilitation Nursing, 35(5), 206–215.
Green, Y. S. (2018). Safety Implications for the Homebound Patient With Dementia. Home Healthcare Now, 36(6), 386. https://doi.org/10.1097/NHH.0000000000000701
Green-McKenzie, J., Gershon, R. R., & Karkashian, C. (2001). Infection Control Practices Among Correctional Healthcare Workers: Effect of Management Attitudes and Availabiity of Protective Equipment and Engineering Controls. Infection Control & Hospital Epidemiology, 22(9), 555–559. https://doi.org/10.1086/501951
Healthy Housing Solutions. (2017). Overcoming Obstacles to Policies for Preventing Falls by the Elderly (Final No. Contract #DU203NP-15-D-06, Order #004). Retrieved from Office of Lead Hazard Control and Healthy Homes; U.S. Department of Housing and Urban Development website: https://portal.hud.gov/hudportal/documents/huddoc?id=OvercomingObstaclesFalls.pdf
Hignett, S., Otter, M. E., & Keen, C. (2016). Safety Risks Associated with Physical Interactions Between Patients and Caregivers During Treatment and Care Delivery in Home Care Settings: A Systematic Review. International Journal of Nursing Studies, 59, 1–14. https://doi.org/10.1016/j.ijnurstu.2016.02.011
Holt-Lunstad, J., Smith, T. B., & Layton, J. B. (2010). Social Relationships and Mortality Risk: A Meta-Analytic Review. PLoS Medicine, 7(7), e1000316.
Hopkins, S., Morgan, P. L., Schlangen, L. J. M., Williams, P., Skene, D. J., & Middleton, B. (2017). Blue-Enriched Lighting for Older People Living in Care Homes: Effect on Activity, Actigraphic Sleep, Mood and Alertness. Current Alzheimer Research, 14(10), 1053–1062. https://doi.org/10.2174/1567205014666170608091119
How Housing Matters original. (2016, March 22). Reengineering Homes for Long-Term Safety and Visitability. Retrieved from https://howhousingmatters.org/articles/reengineering-homes-long-term-safety-visitability/
Hume, R., & Looney, J. (2016, February 3). Designing for Telemedicine Spaces: Planning for the Next Generation of Health Care Delivery. Retrieved October 26, 2016, from Health Facilites Management website: http://www.hfmmagazine.com/articles/1889-designing-for-telemedicine-spaces
Johns Hopkins Hospital at Home. (2015). Hospital at Home History. Retrieved from Hospital at Home website: http://www.hospitalathome.org/about-us/history.php
Keall, M. D., Pierse, N., Howden-Chapman, P., Cunningham, C., Cunningham, M., Guria, J., & Baker, M. G. (2015). Home modifications to reduce injuries from falls in the Home Injury Prevention Intervention (HIPI) study: a cluster-randomised controlled trial. The Lancet, 385(9964), 231–238. https://doi.org/10.1016/S0140-6736(14)61006-0
Kim, I. H., Geiger-Brown, J., Trinkoff, A., & Muntaner, C. (2010). Physically Demanding Workloads and the Risks of Musculoskeletal Disorders in Homecare Workers in the USA. Health & Social Care in the Community, 18(5), 445–455. https://doi.org/10.1111/j.1365-2524.2010.00916.x
Lee, B. C., & Xie, J. (2018). How Do Aging Adults Adopt and Use a New Technology? New Approach to Understand Aging Service Technology Adoption. HCI International 2018 – Posters’ Extended Abstracts, 161–166. https://doi.org/10.1007/978-3-319-92279-9_22
Leff, B., Burton, L., Bynum, J. W., Harper, M., Greenough, W. B., Steinwachs, D., & Burton, J. R. (1997). Prospective Evaluation of Clinical Criteria to Select Older Persons with Acute Medical Illness for Care in a Hypothetical Home Hospital. Journal of the American Geriatrics Society, 45(9), 1066–1073. https://doi.org/10.1111/j.1532-5415.1997.tb05968.x
Leff, B., Burton, L., Mader, S., Naughton, B., Burl, J., Inouye, S. K., … Burton, J. R. (2005). Hospital at Home: Feasibility and Outcomes of a Program To Provide Hospital-Level Care at Home for Acutely Ill Older Patients. Annals of Internal Medicine, 143(11), 798. https://doi.org/10.7326/0003-4819-143-11-200512060-00008
Leff, B., & Madigan, E. (2014, September). The Future of Home Health Care. Presented at the IOM-NRC Workshop, Washington, D.C. Retrieved from https://doi.org/10.17226/21662
Leiss, J. K. (2012). Work Experience, Work Environment, and Blood Exposure among Home Care and Hospice Nurses. Industrial Health, 50, 521–528.
Levine, D. M., Ouchi, K., Blanchfield, B., Diamond, K., Licurse, A., Pu, C. T., & Schnipper, J. L. (2018). Hospital-Level Care at Home for Acutely Ill Adults: a Pilot Randomized Controlled Trial. Journal of General Internal Medicine, 33(5), 729–736. https://doi.org/10.1007/s11606-018-4307-z
Lord, S. R., Hylton, H. B., & Sherrington, C. (2006). Home Environment Risk Factors for Falls in Older People and the Efficacy of Home Modifications. Age and Ageing, 35(suppl_2), ii55–ii59. https://doi.org/10.1093/ageing/afl088
Marcheschi, E., von Koch, L., Pessah‐Rasmussen, H., & Elf, M. (2018). Home setting after stroke, facilitators and barriers: A systematic literature review. Health & Social Care in the Community, 26(4), e451–e459. https://doi.org/10.1111/hsc.12518
Markkanen, P., Quinn, M., Galligan, C., Chalupka, S., Davis, L., & Laramie, A. (2007). There’s No Place Like Home: A Qualitative Study of the Working Conditions of Home Health Care Providers: Journal of Occupational and Environmental Medicine, 49(3), 327–337. https://doi.org/10.1097/JOM.0b013e3180326552
McMurdo, M. E. T., & Gaskell, A. (1991). Dark Adaptation and Falls in the Elderly. Gerontology, 37(4), 221–224. https://doi.org/10.1159/000213264
Meridian at Home: Resources and Tips. (2017). Retrieved February 6, 2017, from Meridian at Home website: http://www.meridianathome.com/mah/index.cfm
Mitka, M. (2001). Home Modifications to Make Older Lives Easier. JAMA, 286(14), 1699–1700. https://doi.org/10.1001/jama.286.14.1699
Mshali, H., Lemlouma, T., Moloney, M., & Magoni, D. (2018). A Survey on Health Monitoring Systems for Health Smart Homes. International Journal of Industrial Ergonomics, 66, 26–56. https://doi.org/10.1016/j.ergon.2018.02.002
N2Care LLC. (2017). MEDCottage. Retrieved March 21, 2017, from MEDCottage website: http://www.medcottage.com/home.html
National Association of Home Builders. (2016). Aging-In-Place Remodeling Checklist. Retrieved October 26, 2016, from https://www.nahb.org/en/learn/designations/certified-aging-in-place-specialist/related-resources/aging-in-place-remodeling-checklist.aspx
National Research Council. (2011). Health Care Comes Home: The Human Factors. Retrieved from https://www.nap.edu/catalog/13149/health-care-comes-home-the-human-factors
O’Brien, M. A., Rogers, W. A., & Fisk, A. D. (2012). Understanding Age and Technology Experience Differences in Use of Prior Knowledge for Everyday Technology Interactions. ACM Transactions on Accessible Computing, 4(2), 27. https://doi.org/10.1145/2141943.2141947
Orpwood, R., Bjørneby, S., Hagen, I., Mäki, O., Faulkner, R., & Topo, P. (2004). User Involvement in Dementia Product Development. Dementia, 3(3), 263–279. https://doi.org/10.1177/1471301204045160
Parker, M. L., Yip, P. M., DeCherrie, L. V., Escobar, C., Fu¨ze´ry, A. K., Price, C. P., & St John, A. (2018). There’s No Place Like Home: Exploring Home-Based, Acute-Level Healthcare. Clinical Chemistry, 64(8), 1136–1142. https://doi.org/10.1373/clinchem.2017.283093
Parsons, K. S., Galinsky, T. L., & Waters, T. (2006). Suggestions for Preventing Musculoskeletal Disorders in Home Healthcare Workers: Part 1: Lift and Transfer Assistance for Paritially Weight-Bearing Home Care Patients. Home Healthcare Nurse, 24(3), 158–164.
Perritt, M., McCune, E., & McCune, S. (2005). Research Informs Design: Empirical Findings Suggest Recommendations for Carpet Pattern and Texture. Alzheimer’s Care Quarterly, 6(4), 300–305.
Polivka, B. J., Wills, C. E., Darragh, A., Lavender, S., Sommerich, C., & Stredney, D. (2015). Environmental Health and Safety Hazards Experienced by Home Health Care Providers: A Room-by-Room Analysis. Workplace Health & Safety, 63(11), 512–522. https://doi.org/10.1177/2165079915595925
Quinn, M. M., Markkanen, P. K., Galligan, C. J., Kriebel, D., Chalupka, S. M., Kim, H., … Davis, L. (2009). Sharps Injuries and Other Blood and Body Fluid Exposures Among Home Health Care Nurses and Aides. American Journal of Public Health, 99(S3), S710–S717. https://doi.org/10.2105/AJPH.2008.150169
Rogers, W. A., & Fisk, A. D. (2010). Toward a Psychological Science of Advanced Technology Design for Older Adults. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 65B(6), 645–653. https://doi.org/10.1093/geronb/gbq065
Simmons-Duffin, S. (2018, January 8). Can Home Health Visits Help Keep People Out of the ER? In Morning Edition. Retrieved from https://www.npr.org/sections/health-shots/2018/01/02/563736154/can-home-health-visits-help-keep-people-out-of-the-er
Sine, D. (2015, February). The Effect of Medical Technology on a Concept of Home. Patient Safety & Quality Healthcare, 18–23.
Span, P. (2018, July 20). Medicare advantage is about to change. Here’s what you should know. The New York Times. Retrieved from https://www.nytimes.com/2018/07/20/health/medicare-advantage-benefits.html?smid=tw-nytnational&smtyp=cur
Tanner, B., Tilse, C., & de Jonge, D. (2008). Restoring and Sustaining Home: The Impact of Home Modifications on the Meaning of Home for Older People. Journal of Housing For the Elderly, 22(3), 195–215. https://doi.org/10.1080/02763890802232048
Taylor, B. J., & Donnelly, M. (2006). Risks to Home Care Workers: Professional Perspectives. Health, Risk & Society, 8(3), 239–256. https://doi.org/10.1080/13698570600871695
Van Hoof, J., & Kort, H. S. M. (2009). Supportive Living Environments: A First Concept of a Dwelling Designed for Older Adults with Dementia. Dementia, 8(2), 293–316. https://doi.org/10.1177/1471301209103276
Wardlow, L. (2018, September 19). Trading Spaces: Remodeling Acute Care for Seniors. Retrieved October 3, 2018, from Institute for Healthcare Improvement website: https://bit.ly/2SbpJc3
Weisfeld, V., & Lustig, T. A. (2015). The Future of Home Health Care: Workshop Summary. Institue of Medicine and National Research Council. Presented at the Forum on Agin, Disability, and Independence, Washington DC. Retrieved from http://ahhqi.org/images/uploads/Home_Health_prepub_NO_EMBARGO_(1)_(1).pdf
Learn about: the homelike model for resident care Riverside Assisted Living Facility Administration wanted to apply, the full-scale mock-ups of the proposed living spaces that launched the project, and the ‘neighborhood’ concept that enables greater resident independence as well as safety.
This webinar offers a once-in-a-lifetime chance to hear from an internationally recognized titan in the field of environments for aging—Dr. Margaret (Maggie) Calkins, and the recipient of 2022 Center for Health Design Changemaker Award—who will share her insights on how design of environments for people as they age has evolved and where the industry is headed.