Advancements in medicine and lifestyle changes have led to an enormous decrease in human mortality worldwide
(Burger, Baudisch, & Vaupel, 2012)
. While life expectancy rates are improving, however, health and quality of life are not
(He, Goodkind, & Kowal, 2016)
. When designing for an aging population, the consensus is that the environment must be prepared for anything. Couldn’t the same be said for any person, at any age? No one knows what tomorrow brings—how an accident or illness could make our comfortable home, our innovative workplace, or our local park completely incompatible with our needs.
Public policies and design strategies tend to focus on meeting the basic safety and physiological needs of older members of society, but there are missed opportunities to support the higher-level needs of all humans. Referencing Maslow’s hierarchy of needs as well as foundational principles of sustainable design, this brief presents a shifting paradigm in the design of environments for aging toward more universal solutions. The universal design approach is being fostered among many forward-thinking groups who see the benefits of equitable, flexible, and accessible design for society as a whole—both today and in the future.
Universal design is being embraced across the built environment. Design strategies include environments that support aging in place, social networks, active living, age-friendly workplaces, and person-centered healthcare. When designing for aging, there are great opportunities at hand to design for ourselves—for every age—for all.
Everyone Is Aging
STATE OF THE AGING WORLD
10,000 people turn 65 every day (Cohn & Taylor, 2010).
By midcentury, the world’s oldest group (85+) will triple in number (Fry, 2016).
In 2020, one in four American workers will be over 55, according to the U.S. Bureau of Labor and Statistics (Fry, 2016).
In 2046, the oldest Millennials will be turning 65 (U.S. Census Bureau, 2015b).
The world’s population is getting older at a rapid rate. Since 1970, the average age of death has increased by 35 years (He et al., 2016). Between now and 2050, the world’s oldest group (aged 80 and over) is projected to more than triple, from 126.5 million to 446.6 million (He et al., 2016). Urgent attention is being paid to this “Silver Tsunami,” making subsequent population waves easy to discount—but a lack of foresight could set us up to be blindsided in a few short years. According to a recent population estimate by the U.S. Census Bureau (2015b), Millennials have recently surpassed Baby Boomers as the nation’s largest generation. Most babies born since 2000 in countries with long life expectancies will live at least 100 years (Christensen, Doblhammer, Rau, & Vaupel, 2009).
While people are living longer, they are not necessarily healthier (He et al., 2016). Worldwide, incidence of multimorbidity increases with age, increasing the need for complex care and use of long-term health services, and adversely impacting quality of life (He et al., 2016). While physical health conditions are often the primary focus when it comes to aging and health, the fallout of cognitive, psychological, and social challenges associated with aging can be just as detrimental. The number of people aged 65 and older with Alzheimer’s disease is projected to nearly triple to 13.8 million by 2050 (Alzheimer’s Association, 2016). Social determinants of health, such as poverty, unemployment, isolation, and discrimination, put older adults at elevated mortality risk (Holt-Lunstad, Smith, & Layton, 2010).
The aforementioned conditions associated with aging have an enormous economic and social impact on society. Families who care for their aging loved ones are often put in a position that forces them to withdraw money from their retirement savings and even cut back on necessities like food (Alzheimer’s Association, 2016). Furthermore, older people are generally dependent on working-age men and women, which could have adverse impacts on the world’s economies (BBC, 2014).
Separate Is Not Equal
The U.S. Supreme Court’s 1954 decision Brown v. Board of Education established the precedent that “separate is not equal.” Even today, however, in the U.S. and many other developed countries, a longstanding tradition continues of building separate, specialized places for aging individuals. In most cases, this is rooted in the best intentions: to ensure that the appropriate environment and health services are immediately available to the people who need them the most. However, these higher-level needs can be met without segregating people according to age. If all environments are designed to meet the needs of aging people, the built environment will be better for everyone.
Paradigm Shift: Aging Issues Are Human Issues
According to Maslow’s hierarchy of needs (Maslow, 1943), a person must address basic physiological and safety needs before pursuing social, esteem, and self-actualization needs (Figure 1). Architects, designers, urban planners, and policy makers tend to focus on how the built environment can support the most basic needs for our youngest and oldest populations, and reserve the designs that support higher-level needs for young and middle-aged adults.
Figure 1: Traditional Approach to Design Over the Life Course based on Maslow's Hierarchy of Needs (Maslow, 1943)
Indeed, environments for more vulnerable (young, old) people must be safe. But why can’t they support social systems, fun, happiness, and inspiration at the same time?
Universal Design
SEVEN PRINCIPLES OF UNIVERSAL DESIGN
Equitable: Useful and marketable to people with diverse abilities.
Flexible: Accommodates a range of preferences and abilities.
Simple and Intuitive: Easy to understand for any user.
Perceptible Information: Communicates information effectively.
Tolerance for Error: Minimizes hazards and unintended actions.
Low Physical Effort: Can be used efficiently and comfortably.
Size and Space: Appropriate for use regardless of the user’s body size, posture, or mobility.
As the number and longevity of older people increases, so does the need for sustainable long-term care and wellness strategies. At the same time, there is a growing need for proactive socioecological systems approaches to total population health and well-being. This continuity in need presents a great opportunity to allow the needs of an aging population to positively impact the design of communities for everyone.
Universal design first appeared in the United States in the 1980s as a means to design for a wider range of users. A decade later, the Center for Universal Design (Story, Mueller, & Mace, 1997) developed a process for defining and evaluating universal design, referred to as the Seven Principles of Universal Design.
The current definition of universal design is quite comprehensive, but in this brief one additional qualifier is proposed to enhance the dynamic applicability:
Universal design is the design of products and environments to be usable by all people, at every changing level of need, to the greatest extent possible, without the need for adaptation or specialized design (Story et al., 1997).
Universal Design Is Sustainable Design
Sustainable design is often associated with “green” design. The design and construction industries have wholeheartedly embraced this approach in many sectors, and increasingly so in design for senior living. However, this shift is not yet fully developed beyond the use of “green” materials. Sustainable design is defined as “the philosophy of designing physical objects, the built environment, and services to comply with the principles of social, economic, and ecological sustainability” (McLennan, 2004). When it is still common practice to build specialized spaces for older generations, moving these individuals from place to place every time their level of need changes, secluding them from society, and forcing emotional and financial burdens on their families, it does not matter how “green” the building materials are; this is not a sustainable solution.
The Triple Bottom Line
The triple bottom line concept originated in the mid-1990s as a means to measure and evaluate business performance. It states that for a business to be successful long-term, it must concurrently address economic, environmental, and social performance outcomes (Elkington, 1998).
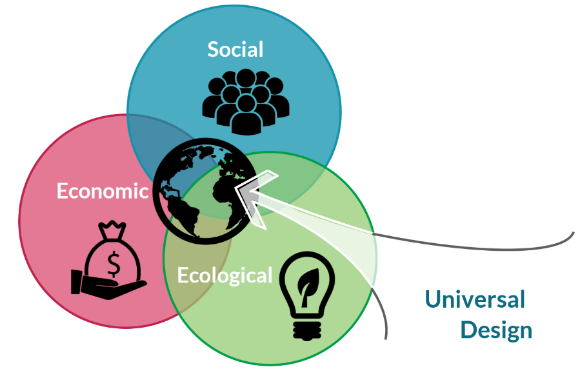
By applying the Seven Principles of Universal Design to a product, a building, or an urban development, one begins to see their alignment with the three components of the triple bottom line. Designers will benefit from referencing the Seven Principles of Universal Design and the triple bottom line iteratively, as the models complement one another well (Figure 2).
Figure 2: Alignment Between Universal Design and Sustainable Design
Universal Design Opportunities
Strategies to address the needs of an aging population must start with shifting paradigms and ageist stereotypes of “old people.” Older individuals are generally considered to be frail, disabled, forgetful, and resistant to change—but in reality, there is large variance within this group, mirroring the diversity of the human population as a whole (Brownell & Kelly, 2013). While roughly one-third of people 65 and older in the U.S. have some type of disability, two-thirds do not (US Census Bureau, 2015a). Strategies to support aging tend to focus on disability and illness, but policy, services, and design should also account for the strengths and assets of older groups.
UNIVERSAL AND SUSTAINABLE DESIGN DEFINED
Universal design is ‘‘the design of products and environments to be usable by all people, to the greatest extent possible, without the need for adaptation or specialized design’’ (Story et al., 1997).
Sustainable design is the philosophy of designing physical objects, the built environment, and services to comply with the principles of social, economic, and ecological sustainability (McLennan, 2004).
This section outlines several innovative design strategies borne out of a need to address challenges faced by aging populations. However, each model incorporates universal design principles and should be considered for the health and well-being benefits for any person at any age. These universal design concepts include case examples across the built environment (home and community, workplace, and healthcare facilities).
Home and Community
The key market for improving accessibility, as well as flexible, adaptable use in the home and nearby community, is the older population (Steinfeld & Maisel, 2012). A recent AARP study (2010) found that 86% of respondents over 45 plan to stay in their current residence as long as possible. The following examples show how design of the home and surrounding community can support this option.
Aging in Place
The Centers for Disease Control and Prevention (2013) defines “aging in place” as the ability to live in one’s own home and community safely, independently, and comfortably, regardless of age, income, or ability. The term has also been used to describe assisted living or long-term care facilities, meaning that after the initial move, residents will not be moved again as their needs change; they will simply receive additional services in the same place.
The “village movement” is growing in many parts of the country as a means to bring different generations together to help aging people remain in their homes instead of moving to “old-age ghettos” (Thomas, 2011). These intergenerational community networks are sometimes formal membership organizations that require a fee for services, and other times more informal and develop out of mutual interest in community sufficiency. Services often include transportation, yard work, bookkeeping, and connections to younger neighbors or youth groups. Aging people are able to receive a menu of assistance similar to what they would receive in a retirement community, but without having to move. Younger generations benefit from building relationships with older members in their communities and considering how similar models might meet their own needs later in life.
Social Networks
As people grow older and move into retirement, they tend to have fewer social networks, and the risk of loneliness and isolation is heightened. However, income, health, and even perceived quality of neighborhood are linked to loneliness for all age groups (Christakis & Fowler, 2007; King, 2008; Lund, 2003). Studies have found that certain characteristics of the built environment can support opportunities for social interaction (Van den Berg, Kemperman, de Kleijn, & Borgers, 2014). Chief among these characteristics are walkable neighborhoods (amenities within ¼ mile), because when people walk around their community they are more likely to form relationships (Lund, 2003).
Old age is the most unexpected of all things to happen to a man.
–Leon Trotsky (Lev Davidovich Bronstein) (Diary in Exile, 1935)
In order to create opportunities for social capital, many senior living and senior care facilities are partnering with schools and daycares to provide opportunities for intergenerational programming. Intergenerational learning—sharing skills, knowledge, and activities among young and old—can promote understanding, personal development, respect, and social capital (Femia, Zarit, Blair, Jarrott, & Bruno, 2008; See & Nicoladis, 2009). One inspiring example is an intergenerational program in Seattle, where residents of Providence Mount St. Vincent senior care community share the facility with 125 children attending daycare (Jansen, 2016). The hallways and vacant rooms double as the children’s playground, and the common spaces serve as a dance floor for all ages.
Active Living
Numerous studies have shown how the built environment can promote active living (Hooker, Cirill, & Geraghty, 2009; Sallis, 2003; Strath, Isaacs, & Greenwald, 2007). These characteristics include infrastructure such as sidewalks and traffic calming devices, as well as landscaping, land use, and overall aesthetics. A study by Takano et al. (2002) found that older adults were more likely to live longer if they lived in walkable neighborhoods with parks and tree-lined streets. For instance, “green streets” are hypothesized to support community well-being, including physical and mental health, the environment, and the economy. These types of streets are known for their focus on landscape-based features and accommodation of multiple travel modes, particularly walking and bicycling.
Workplace
According to the Pew Research Center, more Americans are working beyond the traditional retirement age of 65 than at any time since the turn of the century (Desilver, 2016). As the number of aging workers increases, employment policies and organizational practices are shifting to support more age-friendly work environments. Many of these age-friendly policies attempt to address ageist, abusive, hostile treatment that older workers and persons with disabilities often face due to pervasive stereotypes (Brownell & Kelly, 2013). However, many employers are also making proactive attempts at recognizing that when the culture and environment are positive and supportive of everyone, productivity and quality of work are higher (Brownell & Kelly, 2013). Strategies that aim to support age-friendly work environments are clearly beneficial to workers of all ages.
“If it’s senior-friendly, guess what, it’s people friendly.”
–Dr. Daniel Sewell (Parente, 2015)
Healthcare
In order to better address the complex healthcare needs of older patients, many innovative care models for aging are shifting their improvement efforts toward a person-centered approach. For instance, Sweden’s Esther model was inspired by the unpleasant and potentially dangerous healthcare experience of one woman, “Esther,” a typical older patient who had complex care needs that involved a variety of providers in a variety of settings. Instead of a traditional focus on process improvement, the central concept behind this model is always “What is best for Esther?” Many healthcare organizations who have adopted the Esther model provide extensive personalized care: for instance, having staff meet discharged patients at home to ensure they have everything they need. While outcomes from this model still require further research, program leaders have noted that hospital readmissions have dropped after this model was implemented (Gray, Winblad, & Sarnak, 2016).
A truly patient-centered model means considering how patient recovery extends beyond the walls of the healthcare facility. The “Hospital at Home” model offers patients who are sick enough to be hospitalized but stable enough to be treated at home the latter option (Klein, Hostetter, & McCarthy, 2016). Under the right circumstances (health status and accessible home design), this approach can produce better health outcomes at a lower cost than hospital care (Klein et al., 2016).
Given the complex care needs of aging patients, many emergency departments (EDs) across the nation are embracing strategies that segment older patients into separate treatment tracks. The goal of “geriatric triage” is to provide specialized care for older patients while reducing overall length of stay for patients of all ages (Adams & Gerson, 2003). Additionally, many EDs are working toward “senior-friendly” designs and models of care, including goals such as “environment of respect,” “correct and best procedure and treatment,” and “safe and enabling environment” (Boltz, Parke, Shuluk, Capezuti, & Galvin, 2013). Design can support these goals in a variety of ways: spaces that provide quiet and privacy; high visibility and surveillance; handrails; shock-absorbent flooring; and low beds. While these characteristics are certainly supportive of older adults’ emergency care needs, these features would also benefit anyone in need of emergency care.
Conclusion
While there are several cases of innovative strides toward more universal design, in many cases the basic needs of aging individuals are still not being met. Most buildings and public environments fail to support anything beyond the needs at the lower end of Maslow’s pyramid (Sinclair & Watson, 2014). At the time this brief is being written, the U.S. government is in the midst of confirming the final rule for nursing homes, which will implement changes for long-term care facilities that “reflect the substantial advances that have been made over the past several years in the theory and practice of service delivery and safety” (Centers for Medicare and Medicaid Services (CMS), 2015, p. 1). These changes outline a variety of basic human rights, such as requiring that facilities investigate and report all allegations of abusive conduct (CMS, 2015). Given that the new rules—which should have been implicit decades ago—are being touted as a “major step forward” (Hersher, 2016), there is clearly a long road ahead.
The fact is that everyone is aging—and everyone who is fortunate enough to become a member of the “older population” gets there more rapidly than expected. There is an opportunity at hand for design to support the advancing needs of people as they age. As the numerous examples in this brief show, universal design has the potential to bridge the gap between basic human rights and higher human needs—for everyone.
For Additional Details
For more information on aging populations, visit The Center for Health Design’s website and refer to the Affiliate+ program resources:
AARP. (2010, November). Home and Community Preferences of the 45+ Population [AARP Research]. Retrieved October 5, 2016, from http://www.aarp.org/research/topics/community/info-2014/home-community-services-10.html
Adams, J. G., & Gerson, L. W. (2003). A New Model for Emergency Care of Geriatric Patients. Academic Emergency Medicine, 10(3), 271–274. https://doi.org/10.1197/aemj.10.3.271
Alzheimer’s Association. (2016). 2016 Alzheimer’s disease facts and figures. Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association, 12(4), 459–509.
BBC. (2014, January). A Look Ahead to an Ageing Population [BBC News]. Retrieved from http://www.bbc.co.uk/news/magazine-25968269
Boltz, M., Parke, B., Shuluk, J., Capezuti, E., & Galvin, J. E. (2013). Care of the Older Adult in the Emergency Department: Nurses Views of the Pressing Issues. The Gerontologist, 53(3), 441–453. https://doi.org/10.1093/geront/gnt004
Brownell, P., & Kelly, J. J. (Eds.). (2013). Ageism and Mistreatment of Older Workers. Dordrecht: Springer Netherlands. Retrieved from http://link.springer.com/10.1007/978-94-007-5521-5
Burger, O., Baudisch, A., & Vaupel, J. W. (2012). Human mortality improvement in evolutionary context. Proceedings of the National Academy of Sciences, 109(44), 18210–18214. https://doi.org/10.1073/pnas.1215627109
Centers for Disease Control and Prevention. (2013). Healthy Places Terminology [CDC Healthy Places]. Retrieved October 5, 2016, from https://www.cdc.gov/healthyplaces/terminology.htm
Centers for Medicare and Medicaid Services (CMS). Medicare and Medicaid Programs; Reform of Requirements for Long-Term Care Facilities (Proposed Rule), CFR Parts 405, 431, 447, 482, 483, 485, and 488 Federal Register (2015). Retrieved from https://s3.amazonaws.com/public-inspection.federalregister.gov/2015-17207.pdf
Christakis, N. A., & Fowler, J. H. (2007). The Spread of Obesity in a Large Social Network Over 32 Years. New England Journal of Medicine, 357(4), 370–379.
Christensen, K., Doblhammer, G., Rau, R., & Vaupel, J. W. (2009). Ageing populations: the challenges ahead. The Lancet, 374(9696), 1196–1208.
Cohn, D., & Taylor, P. (2010, December 20). Baby Boomers Approach 65 – Glumly. Retrieved from http://www.pewsocialtrends.org/2010/12/20/baby-boomers-approach-65-glumly/
Desilver, D. (2016). More Older Americans Are Working, and Working More, Than They Used To [Pew Research Center]. Retrieved from http://www.pewresearch.org/fact-tank/2016/06/20/more-older-americans-are-working-and-working-more-than-they-used-to/
Elkington, J. (1998). Cannibals with Forks: Triple Bottom Line of 21st Century Business: Oxford, UK: Capstone Publishing. Retrieved from https://www.amazon.com/Cannibals-Forks-Triple-Century-Business/dp/1841120847
Femia, E. E., Zarit, S. H., Blair, C., Jarrott, S. E., & Bruno, K. (2008). Intergenerational Preschool Experiences and the Young Child: Potential Benefits to Development. Early Childhood Research Quarterly, 23(2), 272–287. https://doi.org/10.1016/j.ecresq.2007.05.001
Fry, R. (2016, April 25). Millennials Overtake Baby Boomers as America’s Largest Generation. Retrieved September 21, 2016, from http://www.pewresearch.org/fact-tank/2016/04/25/millennials-overtake-baby-boomers/
Gray, B., Winblad, U., & Sarnak, D. O. (2016). Sweden’s Esther Model: Improving Care for Elderly Patients with Complex Needs [The Commonwealth Fund Publications - Case Studies]. Retrieved October 3, 2016, from http://www.commonwealthfund.org/publications/case-studies/2016/sep/sweden-esther-case-study
He, W., Goodkind, D., & Kowal, P. (2016). An Aging World: 2015 (International Population Reports No. P95/16-1) (pp. 1–175). US Census Bureau. Retrieved from https://www.census.gov/content/dam/Census/library/publications/2016/demo/p95-16-1.pdf
Hersher, R. (2016, September 29). New Rule Preserves Patients’ Rights to Sue Nursing Homes In Court. The Two-Way. National Public Radio. Retrieved from http://www.npr.org/sections/thetwo-way/2016/09/29/495918132/new-rule-preserves-patients-rights-to-sue-nursing-homes-in-court
Holt-Lunstad, J., Smith, T. B., & Layton, J. B. (2010). Social Relationships and Mortality Risk: A Meta-Analytic Review. PLoS Medicine, 7(7), e1000316.
Hooker, S. P., Cirill, L. A., & Geraghty, A. (2009). Evaluation of the Walkable Neighborhoods for Seniors Project in Sacramento County. Health Promotion Practice, 10(3), 402–410. https://doi.org/10.1177/1524839907307887
Jansen, T. R. (2016, January 20). The Preschool Inside a Nursing Home. The Atlantic. Retrieved from http://www.theatlantic.com/education/archive/2016/01/the-preschool-inside-a-nursing-home/424827/
King, D. (2008). Neighborhood and Individual Factors in Activity in Older Adults: Results from the Neighborhood and Senior Health Study. Journal of Aging and Physical Activity, 16(2), 144.
Klein, S., Hostetter, M., & McCarthy, D. (2016). The Hospital at Home Model: Bringing Hospital-Level Care to the Patient. Retrieved October 5, 2016, from http://www.commonwealthfund.org/publications/case-studies/2016/aug/hospital-at-home?utm_source=Klein+Hospital+At+Home&utm_medium=Twitter&utm_campaign=Delivery+System+Reform
Lund, H. (2003). Testing the Claims of New Urbanism: Local Access, Pedestrian Travel, and Neighboring Behaviors. Journal of the American Planning Association, 60(4), 414–429.
Maslow, A. H. (1943). A Theory of Human Motivation. Psychological Review, 50(4), 370–396. https://doi.org/10.1037/h0054346
McLennan, J. F. (2004). The Philosophy of Sustainable Design (First Edition). Kansas City, MO: Ecotone Publishing Company LLC.
Parente, M. (2015, November 10). There’s No Place Like ... the Hospital? The San Diego Union Tribune. Retrieved from http://www.sandiegouniontribune.com/lifestyle/sdut-ucsd-senior-facility-2015nov10-story.html
Sallis, J. (2003). New Thinking on Older Adults’ Physical Activity. American Journal of Preventive Medicine, 25(3), 110–111. https://doi.org/10.1016/S0749-3797(03)00186-7
See, S. T. K., & Nicoladis, E. (2009). Impact of Contact on the Development of Children’s Positive Stereotyping about Aging Language Competence. Educational Gerontology, 36(1), 52–66. https://doi.org/10.1080/03601270903018352
Sinclair, D., & Watson, J. (2014). Making our Communities Ready for Ageing - A Call to Action (ILC-UK and Age UK Seminar Series) (pp. 1–59). International Longevity Centre - UK. Retrieved from http://www.ilcuk.org.uk/index.php/publications/publication_details/community_matters_making_our_communities_ready_for_ageing_a_call_to_action
Steinfeld, E., & Maisel, J. (2012). Universal Design: Creating Inclusive Environments. Hoboken, N.J.: John Wiley & Sons.
Story, M. F., Mueller, J. L., & Mace, R. L. (1997). The Universal Design File: Designing for People of All Ages and Abilities (Revised). NC State University, The Center for Universal Design. Retrieved from http://eric.ed.gov/?id=ED460554
Strath, S., Isaacs, R., & Greenwald, M. J. (2007). Operationalizing Environmental Indicators for Physical Activity in Older Adults. Journal of Aging and Physical Activity, 15(4), 412.
Takano, T., Nakamura, K., & Watanabe, M. (2002). Urban Residential Environments and Senior Citizens’ Longevity in Megacity Areas: The Importance of Walkable Green Spaces. Journal of Epidemiology and Community Health, 56(12), 913–918.
Thomas, M. (2011). Villages Help Older People Age in Place. AARP The Magazine, (May/June), 1–4.
Trotsky, L. (1935). Diary in Exile. Cambridge: Harvard University Press.
U.S. Census Bureau. (2015a). American Community Survey (ACS). Retrieved October 7, 2016, from https://www.census.gov/programs-surveys/acs
U.S. Census Bureau. (2015b). Population Estimates. Retrieved September 21, 2016, from http://www.census.gov/popest/data/datasets.html?eml=gd&utm_medium=email&utm_source=govdelivery
Van den Berg, P., Kemperman, A., de Kleijn, B., & Borgers, A. (2014). Ageing and loneliness: The role of mobility and the built environment. Travel Behaviour and Society, 5, 48–55. https://doi.org/10.1016/j.tbs.2015.03.001
Learn about: common age-related changes in physical abilities, frequently occurring age-related sensory changes, and supportive adjustments to the physical environment that compensate for functional loss.
In this workshop, expert faculty will share current physical, mental and societal challenges posed when individuals age, discuss programming and design interventions that can assist people (and their care givers) with those challenges, and present case studies and examples that integrate architecture, design and technology into healthy, safe living environments.


 universal solutions. The universal design approach is being fostered among many forward-thinking groups who see the benefits of equitable, flexible, and accessible design for society as a whole—both today and in the future.
universal solutions. The universal design approach is being fostered among many forward-thinking groups who see the benefits of equitable, flexible, and accessible design for society as a whole—both today and in the future.
