By 2031, the largest segment of the U.S. population—the Baby Boom generation—will reach the age of 85 (Alzheimer’s Association, 2018; Crimmins, 2015). At this age, people experience the greatest number and most extreme effects of the normal changes associated with aging. It is also the age associated with the highest risk of developing dementia, particularly Alzheimer’s disease and LATE (limbic-predominant age-related TDP-43 encephalopathy) (Alzheimer’s Association, 2018; Crimmins, 2015; Nelson et al., 2019).
PROGRAMMING CONSIDERATIONS FOR MEMORY CARE DESIGN:
Integrated care
Interconnections with the surrounding community
Small building scale with fewer occupants
Intuitive layout of rooms, adjacencies, and affordances
Destination-based amenities and services
Access to nature
Residential ambiance, character, and décor
Access to familiar items, equipment, and tools
Regulation of contextual sensory stimulation
Involvement in meal planning and preparation
Spa-like bathing atmosphere
Single bedrooms for comfort, privacy, and personalization
Currently, there is no prevention, cure, or therapy for Alzheimer’s or LATE (Alzheimer’s Association, 2018; Nelson et al., 2019; World Health Organization [WHO], 2018). People with dementia frequently experience an alternate reality and exhibit maladaptive behavioral responses; the use of physical and chemical restraints to control many of the most problematic and pervasive symptoms is restricted by regulating agencies. (See Appendix B for more detail.) Accordingly, the development of truly effective interventions required designers and care givers to “go into the world” of those with dementia to try to understand the nature of the messages that they express and effectively address the source of their behavior. To this end, environmental design can have a profound effect on the quality of life and care for older adults (Scales, Zimmerman, & Miller, 2018). The built environment can reduce the stresses associated with declining physical abilities, memory loss, and care provision.
It is important to understand the changes associated with normal aging, as well as the changes common to dementia. Understanding the unique abilities and challenges of these populations better equips teams to design supportive living spaces that can serve as therapeutic resources for both individuals aging normally and those living with Alzheimer’s and other dementias. The literature suggests 12 programming considerations for design to support these populations and demonstrates how these design principles, while particularly relevant for people with impairments, can benefit everyone (Nahemow & Lawton, 1973).
Background
The unprecedented number of people living to the age of 85 and older continues to provide designers with opportunities and challenges to devise critical, creative, enabling, sustainable, and adaptive solutions. One area of increasing interest is the role environmental strategies can play in supporting the normal changes associated with aging along with the many forms of dementia, including Alzheimer’s disease (Calkins, 2018; Chaudhury et al., 2017; Flinner et al., 2018; Hitzig & Sheppard, 2017; Lorusso & Bosch, 2017; Morgan et al., 2012; Parke et al., 2016; Scales et al., 2018). However, it can be difficult for care providers and designers, who observe and approach these conditions with a degree of professional detachment, to comprehend the kinds of changes that may be encountered.
Understanding Alzheimer’s Disease and Other Dementias
While the process of aging is accompanied by many physiological changes, memory loss and confusion are no longer accepted by physicians, psychologists and sociologists as a “normal” part of growing older (Hodes, 2007). Despite this, it is becoming increasingly common to know someone who has (or had) dementia. Unlike cancer, cardiac conditions, and other diseases, there are not yet any reliable or proven treatment options to slow or stop the progression of many types of dementia (Alzheimer’s Association, 2018; Nelson et al., 2019; WHO, 2018).
“Dementia,” in fact, is not a disease. It’s an umbrella term used to describe a set of symptoms (Alzheimer’s Association, 2018). At least two of the five core mental functions have to be significantly impaired for an individual to be diagnosed with dementia:
Memory
Communication
Reasoning
Concentration
Perception
Alzheimer’s is a degenerative brain disease that typically begins years before the symptoms become apparent (Alzheimer’s Association, 2018). LATE (limbic-predominant age-related TDP-43 encephalopathy) is a newly discovered type of dementia which was previously confused with Alzheimer’s. It is now known that it affects 20–50% of people older than 80 (Nelson et al., 2019). Alzheimer’s and LATE are often comorbid and are the most common cause of dementia, accounting for 60–80% of cases. The hallmark of these types of dementia is damage and destruction to the areas of the brain that effect memory and enable basic bodily functions such as walking and swallowing (Alzheimer’s Association, 2018; Nelson et al., 2019). Symptoms advance from mild to moderate to severe at different rates based on the individual (Alzheimer’s Association, 2018).
ACTIVITIES OF DAILY LIVING (ADLs)
Hygiene: Bathing, showering, grooming, nail and oral care
Dressing: Dressing and undressing oneself
Eating: Feeding oneself (and, in some cases, preparing food)
Continence: Cleaning oneself and carrying out toileting tasks
Ambulation: Standing, sitting, walking, and getting in and out of bed
Dementia can be caused by various diseases, strokes, head injuries, drugs, and even nutritional deficiencies. On average, 40% of the people who live into old age will develop some type of dementia (Alzheimer’s Association, 2018). One person is diagnosed with dementia every three seconds. Women over the age of 65 are twice as likely as men to develop dementia, and certain biomarkers can be detected decades before the onset of some dementias (Alzheimer’s Association, 2018). Individuals who do not develop dementia are likely to be responsible for providing dementia care in some capacity. (See Appendix A for more detail.)
Changes Associated with Normal Aging and Dementia
Understanding the unique abilities and challenges faced by aging individuals, especially those living with dementia, better equips teams to design supportive living spaces. Aging individuals are evaluated based on their ability to perform general activities of daily living (ADLs) and instrumental activities of daily living (IADLs) (Finlayson, Mallinson, & Barbosa, 2005). ADLs include five general categories of activities that must be carried out on a daily basis in order for a person to live independently at home or in the community. IADLs refer to seven categories of activities which may not be essential on a daily basis, but are still viewed as important features of independent living.
Normal Age-Related Changes
Normal age-related changes include weakened bones and joints; decreased muscle mass; slowed digestion and metabolism; bowel and bladder incontinence; dental and gum conditions; thin and fragile skin; poor balance, coordination, and reflexes; impaired, distorted, or tinted vision; and diminished or distorted hearing (Hodes, 2007).
Around the age of 40–50, muscle tissue starts to decrease and osteoporosis begins to weaken bones to the point where they break easily. This decline becomes more pronounced after 60. Half of all people aged 65 and older experience arthritic inflammation, pain, swelling, and joint stiffness.
Digestive complications arise as aging bodies process food, eliminate waste, and use energy differently. These issues can be compounded by poor oral health (problems with bones, gums, and the decay or loss of teeth). While aging alone does not cause incontinence, at least 1 in 10 people over age 65 has incontinence, often women.
Skin becomes thinner and loses underlying fatty tissue with age, making it increasing fragile, prone to injury, and sensitive to temperature changes. Wrinkles, dryness, and pigmentation spots also increase.
Falls become increasingly common as coordination, muscle mass, and reflexes are affected by age-related changes to sight, hearing, strength, illness, and reactions to medications.
At about 40 years old, eyesight weakens, and by 60, cataracts and macular degeneration may develop. Small print becomes more difficult to read, and some people experience obscured or clouded vision, vision loss, or blindness. The lens of the eye also begins to turn yellow, changing the perception of color.
About one-third of Americans aged 65–74 have hearing problems, and about half of people over 85 have hearing loss. A decline in hearing may be accompanied by internal ringing, roaring, or other noises.
Figure 1: Normal Age-Related Changes
In the past, memory loss and confusion were accepted as a normal part of growing older; although it may take longer to remember things, individuals can remain both alert and competent in old age.
Changes Associated with Alzheimer’s Disease and Other Dementias
Changes credited to dementia are noticeably different from those of normal aging. According to the Alzheimer’s Association (2018), changes associated with dementia include disruptive memory loss; impaired judgment and recall; confusion over time and place; misunderstanding imagery/spatial relationships; challenges in planning, problem solving, and completing familiar tasks; social withdrawal; language difficulties; and changes in mood and personality. One of the most common signs of dementia is memory loss to the degree that it disrupts daily life, especially forgetting recently learned information or important dates and events, as well as losing items or placing them in unusual locations without the ability to recover them by retracing steps.
Figure 2: Alzheimer’s Disease and Other Dementias
Those with Alzheimer’s may also have trouble following or joining a conversation, unexpectedly stopping, trailing off, or inappropriately interrupting. They may struggle with vocabulary, have problems finding the right word, or call things by the wrong name. In addition to changes in judgment and decision-making, this can lead to repetitive questions, as well as accusations of lying, keeping secrets, or stealing. For some people, vision problems such as difficulty reading, judging distance, or determining color or contrast are signs of Alzheimer’s. The confusion, suspicion, depression, fear, and anxiety that results from information that exceeds the processing or participation abilities of individuals with dementia often leads to withdrawal from activities and social situations. (See Appendix B for more detail.)
A Smart Investment Through Design
Therapeutic features should be considered at a variety of environmental scales and locations in evidence-based design interventions for individuals with dementia. Goal- and evidence-based solutions are prudent investments that support efficiency, efficacy, and cost savings in the provision of high-quality care and living experiences (Gramegna & Biamonti, 2017). Moreover, these solutions enable designers to prioritize decisions that are in the best interest of those living and working in care settings, rather than preemptively constraining opportunities with less permanent limitations (e.g., codes, regulations, practices, and personnel) that may change in the near or distant future. The design-based evidence for advancing therapeutic goals for supportive memory care settings includes 12 environmental programmatic strategies, each outlined below.
Integrating Memory Care
Enable interactions between those with and without dementia
People with dementia are frequently denied the basic rights and freedoms available to others on the grounds that their impairments are inherently disabling (Calkins, 2018). However, more people are receiving their diagnosis earlier, living into old age, and living longer within old age (Alzheimer’s Association, 2018). New understandings of what constitutes disability are being established thanks to the self-organization and activism of individuals with Alzheimer’s disease and other dementias who are unwillingly being disabled, stigmatized and marginalized (Calkins, 2018).
In the past, the vast majority of design and medical professionals believed individuals living with dementia had distinct and unique needs in comparison with other residents in long-term care settings (Calkins, 2018; Chaudhury et al., 2017). In contrast with traditional, highly institutional buildings and care practices, the design of Alzheimer’s special care units (SCUs) was based on advancing therapeutic goals for a small number of people in a place that felt more like home. Regardless of age or dementia, almost everyone’s functional abilities are affected at some point in their lifetime. Those who survive to old age are increasingly likely to experience multiple functional difficulties, particularly those experiencing dementias. Consequently, these strategies are equally applicable to any individual in long-term care (Calkins, 2018).
Although the development of segregated living areas solely for individuals living with dementia continues, there is increasing discussion that segregation contributes to the stigma associated with a dementia diagnosis and that individuals living with dementia should be enabled to live alongside those who do not currently have dementia. Beyond the stigmatization, this kind of integration makes sense given that 40% of assisted living residents and 60% of nursing home residents have moderate to severe cognitive impairment (Calkins, 2018). Increasingly, from a regulatory perspective, there is also discussion around whether or not to interpret a secured unit as a restraint.
Considering the broad and frequent use of all healthcare options and settings by individuals with dementias (Appendix C), it stands to reason that environmental strategies could be successfully applied across the continuum of care, as well as in private residences, community settings, hospitality hubs, and beyond (Alzheimer’s Association, 2018; Crimmins, 2015; Hebert et al., 2013; Nelson et al., 2019).
Facilitate contact and engagement with the surrounding community
A movement referred to as “dementia-friendly communities” has been gaining traction around the globe, largely focusing on educating commercial and service employees to understand and support individuals with dementias
(WHO, 2018)
. Some U.S. communities are following suit by providing access to the surrounding residential community or by bringing the surrounding community into the care setting
(Calkins, 2018)
.
Reducing Scale
Reduce the perceived size and number of occupants per care space (e.g., living spaces, bedrooms)
Regardless of building configuration, designers and care providers are devising environmental and service models that capitalize on the intimate and familiar nature of the household model (Calkins, 2018; Chaudhury et al., 2017; Flinner et al., 2018). While some approaches, such as Green House homes, provide parameters for decision-making, the vast majority are being tailored to the needs and desires of care providers and their constituents.
Simplifying the Layout
Design intuitive room configurations, adjacencies, and affordances
Long-term care settings originally gained a financial foothold as an extension of acute care and, accordingly, were built in the same style. There is, however, an inherent misfit for individuals trying to live for long periods of time in an environment intended for a short-term and care-dependent population. Unlike traditional, institutional buildings that focus on service delivery, residential-style settings afford the opportunity to locate bedrooms farther away from frequently accessed and occupied shared spaces. Similarly, the presence of a fireplace, animals, music, and other familiar household affordances sends a consistent message that this is a home to be lived in, rather than an institution or unit to escape from (Calkins, 2018).
The best way to prevent falls, incontinence, and pressure ulcers is to keep people moving—a goal that can only be achieved by designing environments with distances perceived to be manageable. One valuable resource is the six-minute walk test (6MWT), which measures the total distance an individual is able to walk in six minutes on a hard, flat surface. This physical and occupational therapy exercise (along with vision limitations) can help designers to determine the maximum distance between destinations, such as a bedroom and a dining area (Liu et al., 2016).
There is an inherent misfit for individuals trying to live for long periods of time in an environment intended for a short-term and care-dependent population.
When new construction is not an option and long hallways are unavoidable, codes now allow for seating in an 8’ corridor (Carson, 2013). Intermediate seating provides an opportunity to subdivide a long (seemingly unmanageable) distance into several shorter, more manageable distances.
Including Destinations
Capitalize on amenities, venues, and services
Expectations around what is and isn’t appropriate/desirable in long-term care settings are changing. On-site and easily accessible destinations, attractions, and venues appeal not only to older adults as ways to connect with others, but also to their children as entertainment options when visiting
(Hitzig & Sheppard, 2017)
. Multi-purpose rooms with folding tables and storage cabinets full of games are no longer marketable as a value-added proposition.
Many care providers are trying to gain a competitive edge by catering to the preferences of future clientele. Child-friendly spaces are an overlooked but popular option, providing children with a comfortable environment that is safe without being overly restrictive. Spaces for kids may be inside or out, depending on the preferences of the care provider and clients
(Calkins, 2018)
. Options for reliable transportation are a priority for many communities to allow individuals ongoing access to community-based services such as doctor’s offices and shops.
Accessing Nature
Offer access to natural settings, features, and activities
Outdoor spaces are often untapped or under-utilized opportunities to extend programming and activities
(Calkins, 2018; Chaudhury et al., 2017; Scales et al., 2018)
. Exterior features offer possibilities that cannot be achieved inside, such as large-group functions, gardening, and grilling. Care must be taken, naturally, to design out any dangers that may be present, but taking advantage of outdoor spaces is well worth the effort.
Because of the many benefits associated with access to nature, these opportunities should be capitalized upon regardless of location. The selection of quality and durable materials is important, with an emphasis on those able to withstand intense climate conditions. When going outside is not an option or an alternative is preferred, verandas and atriums are attractive solutions that offer unique programming opportunities as well as afford year-round access.
Maximizing Familiarity
Accentuate residential ambiance, character, and décor
It is highly beneficial to individuals with dementias to be surrounded by a context that does not exceed their capacity for understanding how to appropriately engage with others or the setting. When pushed beyond their coping threshold, many individuals exhibit maladaptive behaviors. Armed with this knowledge, designers can better support individuals’ functioning and quality of life.
THE IMPORTANCE OF FAMILIARITY
It is highly beneficial to individuals with various kinds of dementias to be surrounded by a context that does not exceed their capacity for understanding how to appropriately engage with others or the setting. When pushed beyond their coping threshold, many individuals exhibit maladaptive behaviors.
There should be seating to accommodate people of a variety of shapes and sizes, but not so much furniture that those who use wheelchairs or motorized ambulatory aids feel excluded from a seating area
(Calkins, 2018)
. To recreate a homelike feel, decorative items and furniture may be somewhat eclectic, especially if residents are encouraged to personalize spaces with their own possessions
(Parke et al., 2016)
. Healthcare equipment should be stored in discreet but accessible locations, ideally out of sight
(Calkins, 2018; Chaudhury et al., 2017; Flinner et al., 2018)
. Special considerations often have to be made for electrical access to motorized lifts. Floor, wall, and ceiling finishes should have a residential look, but commercial-grade durability and sound absorption.
Prioritizing Access to Everyday Items
Provide access to commonly used amenities, equipment, and tools
Providing varying degrees of access to household items is also appropriate. The important part is determining which items are familiar and of interest. In the case of some activities, like cooking, gardening, or painting, there is the added benefit of active and passive participation (Calkins, 2018; Chaudhury et al., 2017). Creating areas for individuals to spontaneously engage in such activities is also an effective strategy (Hitzig & Sheppard, 2017). While this strategy goes by many names (e.g., “prepared environment”), the unifying theme is providing opportunities for unplanned and unsupported engagement.
Regulating Sensory Stimulation
Controlling the presence, absence, or type of contextual stimulation
Sensory stimulation is a popular term, but discussions would be better framed around the regulation of stimulation. Every single source of stimulation should be carefully considered to avoid any byproducts of a careless design or value engineering process.
Every single source of stimulation should be carefully considered to avoid any byproducts of a careless design or value engineering process.
Vision
Treatment of low vision and other visual disorders is a medical issue; assuring optimal access to the built environment for persons with visual impairments is a design issue. Visual cues in the architecture and interior design of a space aid in interactions with surroundings. Lack of clarity in visual cues, along with any defects in interpretation or comprehension of the environment, can reduce the ability to understand and safely navigate the environment (NIBS [National Institute of Building Sciences], 2013). Regardless of cognition abilities, vision deficits common in aging individuals can impact their ability to clearly see and interpret their environment (Figueiro, Plitnick, Rea, Gras, & Rea, 2011). This should inform the physical layout of spaces and the configuration of furnishings.
Considerations related to color selection should account for the yellowing lenses of the aging eye. Subtle variations, and even some colors that are markedly different from one another, can be difficult to distinguish.
Acoustics
Noise contributes to physical and psychological disability. Figure 3 depicts recommended sound levels for shared spaces (40 dB) and bedrooms (20 dB). The actual average volume within long-term care (LTC) settings for both of these spaces is much louder at approximately 57 dB, regardless of the time of day (Bharathan et al., 2007; Sykes, Tocci, & Cavanaugh, 2013).
Figure 3: Recommended vs. actual long-term care sound levels and associated consequences.
While sounds at 40–50 dB are not known to cause permanent hearing damage , ongoing exposure has been linked to emotional and physiological reactions, disturbed sleep, and delirium, and can negatively impact work performance (Bharathan et al., 2007; Sykes et al., 2013). An increase to 55–60 dB creates an environmental stressor triggering an acute and chronic increase in “fight-or-flight” and “defeat” reactions. Noise pollution disproportionately affects older adults, especially those with dementia.
In order to accurately hear, interpret, and participate in conversations, older adults require an increase of 10–15 dB in the volume of speech, resulting in a 30 dB increase above ambient conditions (Bharathan et al., 2007). This helps to explain why those without impaired hearing feel as though they are yelling to be heard and experience difficulty participating in conversations.
Insulated drywall, acoustic ceiling tiles, carpeted floors, wireless pagers, lubricated hinges, private bedrooms, and clinical offices (instead of stations) can improve the acoustics of spaces, improving sleep, focus, mood, strength, stamina, diet, and work performance.
Enhancing Meals
Maximize involvement in meal planning, preparation, and service
Just because a person has lost their ability to recall specific events or details does not mean they have lost their ability to enjoy good food. Accessible, fully functional kitchens with considerations for acoustics and safety are an ideal resource for activities and meal preparation within settings for dementia care
(Calkins, 2018)
. Other community-based dining, café, and convenience options offer additional variety and novelty.
Providing a Spa Experience
Optimize bathing location, layout, fixtures, décor, and storage
Historically, SCUs have tried to minimize behavioral outbursts associated with bathing individuals with dementia. After “failing forward” for many years, it is now understood that avoiding negative behaviors isn’t the same as promoting positive experiences (Calkins, 2018; Chaudhury et al., 2017). For better results, bathing environments should be designed based on an experiential approach.
Bathing is not typically an activity that older adults engage in on a daily basis. Because of this, efforts should be made to optimize the positive features of the bathing experience, such as relaxation. The layout of the setting should prioritize privacy and minimize drafts. Equipment should be selected based on function, access, and aesthetics. Most importantly, the character of the space should be warm, inviting, well-appointed, and clean.
Personalizing Bedrooms
Private bedroom suites afford comfort, privacy, and personalization
All individuals benefit from having private rooms with private, en-suite bathrooms
(Calkins, 2018; Parke et al., 2016; Prizer & Zimmerman, 2018)
. Side-by-side beds with “privacy curtains” compromise an individual’s quality of living, and—some would contend—violate their right to a safe and secure environment
(Calkins, 2018)
. (After all, people are never more vulnerable than when they are sleeping.) Bathrooms, too, are beginning to receive more attention than they have in the past. Privacy is no longer considered a privilege; it’s an expectation. Visual and physical accessibility is especially important in these spaces.
Conclusion
The language used to describe symptoms, behavior, dementia, and aging has important implications for the way that people are considered and treated. Impairments must start to be viewed through more than a deficit-based clinical lens. Advocates and activists are challenging long-held assumptions about the limitations of the elderly and devising enabling alternatives for this population.
In order to design spaces that support and enable aging individuals, especially those with dementias, it is critical to be able to identify and access the most credible, up-to-date, and innovative information for memory care design.
Some of the most overlooked but relevant sources of information are the individuals living with these symptoms. There are ways that individuals with dementia can be successfully engaged—and, as the saying goes, “Practice makes perfect.” The more familiar and comfortable designers become observing and engaging with them, the better equipped they will be to design settings that support and enable older adults, especially those with Alzheimer’s disease and other dementias.
Appendix A
The Global Impact of Dementia
Figure 4: Global Dementia Distribution
The World Health Organization currently estimates that as of 2020, 50 million people have dementia worldwide. That number is projected to grow to 82 million by 2030, and 152 million by 2050 (WHO, 2018). If dementia were a nation, it would have the 18th largest economy in the world. If dementia care were a company, it would have had the world’s largest corporate annual revenue—$610 billion—in 2018, with a workforce of more than 16 million unpaid caregivers in the U.S. alone (WHO, 2018).
National Impact
The age of 85 is critical, as this is the age associated with the highest risk of developing dementia, especially Alzheimer’s disease and LATE (Alzheimer’s Association, 2018; Nelson et al., 2019). In 2018, about 2.1 million people with Alzheimer’s dementia were 85 or older, accounting for 37% of the 5.7 million people in the U.S. with Alzheimer’s-type dementia (Alzheimer’s Association, 2018).
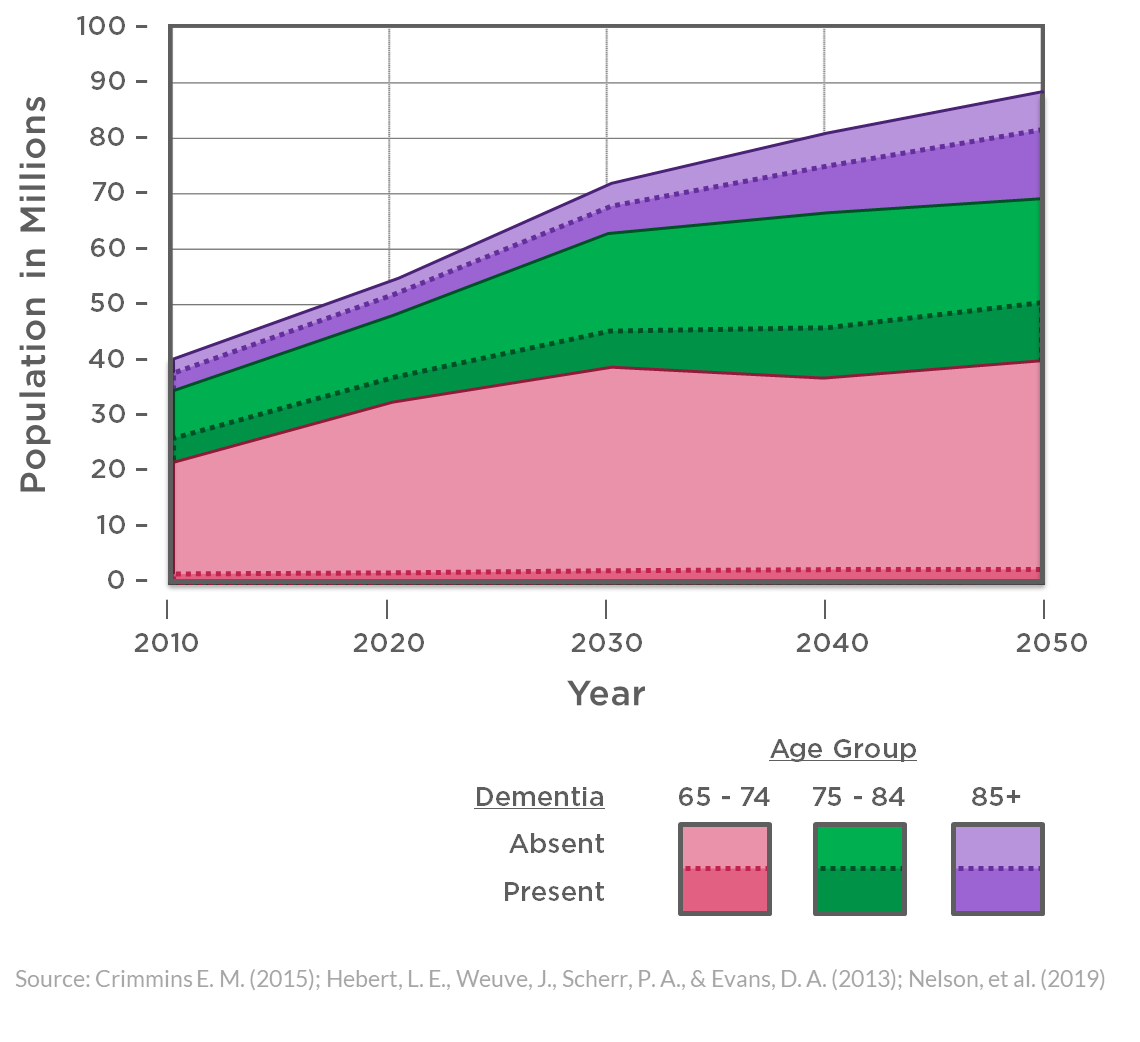
Figure 5: U.S. Population Forecast: People 65+ with Dementia
2031 is seen as a pivotal year, because it is when the first wave of Baby Boomers will reach age 85. At this point, it’s projected that about 3 million people from the previous generation will have Alzheimer’s dementia—an increase of about 1 million people in a little over a decade (Alzheimer’s Association, 2018).
By 2050, 7 million people aged 85 and older are projected to have Alzheimer’s dementia, more than doubling the current population in just under two decades and accounting for over half of all people aged 65 and older with Alzheimer’s dementia (Alzheimer’s Association, 2018).
Appendix B
Symtoms
Alzheimer’s is a degenerative brain disease that typically begins years before the symptoms become apparent. LATE, short for limbic-predominant age-related TDP-43 encephalopathy, is a newly discovered type of dementia that affects 20–50% of people older than 80; it was previously confused with Alzheimer’s due to similarities in symptoms. Alzheimer’s and LATE are often comorbid and are the most common cause of dementia, affecting 60–80% of those with dementia. The hallmark of these types of dementia is damage and destruction to the areas of the brain that effect memory and enable basic bodily functions such as walking and swallowing.
Frontotemporal lobar degeneration, Parkinson’s disease, Vascular dementia, and Lewy bodies tend to be the next most common causes of dementia. Symptoms associated with these types of dementia include visuospatial impairment, motor impairment, slowness, rigidity, gait changes, and imbalance, as well as difficulty constructing or understanding language.
About half of older people with dementia have more than one type, a condition referred to as “mixed dementia.” While the likelihood of mixed dementia increases with age, the pace at which the symptoms advance from mild to moderate to severe varies from person to person.
Figure 6: Prevalence and Problems of Dementia Symptoms
People with dementia experience an alternate and isolated reality. Because they have difficulty interpreting and explaining the sources of their confusion and discomfort, they often express themselves through actions. Eighty-three percent of older adults with a cognition impairment exhibit a variety of behavioral symptoms that affect their own well-being and that of their caregivers (Cunningham, McGuinness, Herron, & Passmore, 2015; Fauth & Gibbons, 2014). Unfortunately, determining which behaviors are the most problematic depends on their prevalence, frequency, and intensity, as well as caregivers’ distress and/or negative caregiver outcomes (Fauth & Gibbons, 2014).
Figure 6 depicts the average prevalence of dementia symptoms and caregivers’ perceived problems associated with these symptoms. Symptoms are listed in descending order based on the combined average.
Appendix C
Impact on Healthcare Services
Seventy percent of older adults with Alzheimer’s and other dementias reside in home- or community-based settings (Alzheimer’s Association, 2018). It is worth noting that the healthcare utilization patterns by those with Alzheimer’s and other dementias tend to have more intense implications than those of other older adults. Beyond the implications for use, many healthcare settings serve a higher proportion of clients with dementias.
IMPACT ON HEALTHCARE SERVICES
More than half of hospital stays for people aged 65+ are associated with Alzheimer’s disease or other dementias.
Hospital in-patient stays are more than 4 times as long for individuals with dementia.
People with dementia are more than twice as likely to have emergency department visits as those without.
Nursing home admissions are 4 times as frequent for people with Alzheimer’s or other dementias.
While transitions from home- and community-based locations to formal healthcare settings are not uncommon toward the end of life, individuals with Alzheimer’s and other dementias make broad use of a variety of healthcare options throughout their lives (Alzheimer’s Association, 2018; Crimmins, 2015; Hebert, Weuve, Scherr, & Evans, 2013; Nelson et al., 2019).
40% of residents in residential care facilities have dementia.
50% of nursing home residents have dementia, and 61% have moderate or severe cognitive impairment.
Alzheimer’s SCUs are dedicated units in nursing homes that have tailored services for individuals with Alzheimer’s or other dementias. Despite 61% of nursing home residents having moderate or severe cognitive impairment, SCUs account for just 4% of all nursing home beds.
References
Alzheimer’s Association. (2018). 2018 Alzheimer’s disease facts and figures. Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association, 14(3), 367–429. https://doi.org/10.1016/j.jalz.2018.02.001
Bharathan, T., Glodan, D., Ramesh, A., Vardhini, B., Baccash, E., Kiselev, P., & Goldenberg, G. (2007). What do patterns of noise in a teaching hospital and nursing home suggest? Noise & Health, 9(35), 31–34.
Calkins, M. P. (2018). From Research to Application: Supportive and Therapeutic Environments for People Living With Dementia. The Gerontologist, 58(suppl_1), S114–S128. https://doi.org/10.1093/geront/gnx146
Carson, C. (2013). Between Clear and Cluttered: The Life Safety Code and health care corridor width. NFPA Journal, (February). Retrieved from https://www.nfpa.org/News-and-Research/Publications-and-media/NFPA-Journal/2013/January-February-2013/The-Experts/In-Compliance
Chaudhury, H., Cooke, H. A., Cowie, H., & Razaghi, L. (2017). The Influence of the Physical Environment on Residents With Dementia in Long-Term Care Settings: A Review of the Empirical Literature. The Gerontologist. https://doi.org/10.1093/geront/gnw259
Crimmins, E. M. (2015). Lifespan and Healthspan: Past, Present, and Promise. The Gerontologist, 55(6), 901–911. https://doi.org/10.1093/geront/gnv130
Cunningham, E. L., McGuinness, B., Herron, B., & Passmore, A. P. (2015). Dementia. The Ulster Medical Journal, 84(2), 79–87. Retrieved from PubMed. (26170481)
Fauth, E. B., & Gibbons, A. (2014). Which behavioral and psychological symptoms of dementia are the most problematic? Variability by prevalence, intensity, distress ratings, and associations with caregiver depressive symptoms. International Journal of Geriatric Psychiatry, 29(3), 263–271. https://doi.org/10.1002/gps.4002
Fazio, S., & Mitchell, D. B. (2009). Persistence of self in individuals with Alzheimer’s disease: Evidence from language and visual recognition. Dementia, 8(1), 39–59. https://doi.org/10.1177/1471301208099044
Figueiro, M. G., Plitnick, B., Rea, M. S., Gras, L. Z., & Rea, M. S. (2011). Lighting and perceptual cues: Effects on gait measures of older adults at high and low risk for falls. BMC Geriatrics, 11, 49–49. https://doi.org/10.1186/1471-2318-11-49
Finlayson, M., Mallinson, T., & Barbosa, V. M. (2005). Activities of daily living (ADL) and instrumental activities of daily living (IADL) items were stable over time in a longitudinal study on aging. Journal of Clinical Epidemiology, 58(4), 338–349. https://doi.org/10.1016/j.jclinepi.2004.10.008
Flinner, J., Kallmyer, B., Pace, D., & Fazio, S. (2018). The Fundamentals of Person-Centered Care for Individuals With Dementia. The Gerontologist, 58(suppl_1), S10–S19. https://doi.org/10.1093/geront/gnx122
Gramegna, S. M., & Biamonti, A. (2017). Environment as non pharmacological intervention in the care of Alzheimer’s disease. The Design Journal, 20(Suppl. 1), S2284–S2292. https://doi.org/10.1080/14606925.2017.1352744
Hebert, L. E., Weuve, J., Scherr, P. A., & Evans, D. A. (2013). Alzheimer disease in the United States (2010-2050) estimated using the 2010 census. Neurology, 80(19), 1778–1783. https://doi.org/10.1212/WNL.0b013e31828726f5
Hitzig, S. L., & Sheppard, C. L. (2017). Implementing Montessori Methods for Dementia: A Scoping Review. The Gerontologist, 57(5), e94–e114. https://doi.org/10.1093/geront/gnw147
Hodes, R. J. (2007). Your Guide to the New Science of Aging Well: 8 Areas of Age-Related Change. NIH MedlinePlus, (Winter), 10–13.
Liu, W.-Y., Meijer, K., Delbressine, J. M., Willems, P. J., Franssen, F. M. E., Wouters, E. F. M., & Spruit, M. A. (2016). Reproducibility and Validity of the 6-Minute Walk Test Using the Gait Real-Time Analysis Interactive Lab in Patients with COPD and Healthy Elderly. PloS One, 11(9), e0162444–e0162444. https://doi.org/10.1371/journal.pone.0162444
Lorusso, L. N., & Bosch, S. J. (2017). Impact of Multisensory Environments on Behavior for People With Dementia: A Systematic Literature Review. The Gerontologist, 58(3), e168–e179. https://doi.org/10.1093/geront/gnw168
Morgan, R. O., Fouladi, N. N., Sail, K. R., Snow, A. L., Davila, J. A., & Kunik, M. E. (2012). Modeling Causes of Aggressive Behavior in Patients With Dementia. The Gerontologist, 53(5), 738–747. https://doi.org/10.1093/geront/gns129
Nahemow, L., & Lawton, M. P. (1973). Ecology and the aging process. In C. Eisdorfer & M. P. Lawton (Eds.), The psychology of adult development and aging (pp. 619–674). Washington, D.C., U.S.: American Psychological Association.
Nelson, P. T., Dickson, D. W., Trojanowski, J. Q., Jack, C. R., Boyle, P. A., Arfanakis, K., … Schneider, J. A. (2019). Limbic-predominant age-related TDP-43 encephalopathy (LATE): Consensus working group report. Brain. https://doi.org/10.1093/brain/awz099
NIBS (National Institute of Building Sciences). (2013). Design Guidelines for the visual environment. https://cdn.ymaws.com/www.nibs.org/resource/resmgr/LVDC/LVDP_Guidelines_052815.pdf
Parke, B., Boltz, M., Hunter, K. F., Chambers, T., Wolf-Ostermann, K., Adi, M. N., … Gutman, G. (2016). A Scoping Literature Review of Dementia-Friendly Hospital Design. The Gerontologist, 57(4), e62–e74. https://doi.org/10.1093/geront/gnw128
Prizer, L. P., & Zimmerman, S. (2018). Progressive Support for Activities of Daily Living for Persons Living With Dementia. The Gerontologist, 58(suppl_1), S74–S87. https://doi.org/10.1093/geront/gnx103
Scales, K., Zimmerman, S., & Miller, S. J. (2018). Evidence-Based Nonpharmacological Practices to Address Behavioral and Psychological Symptoms of Dementia. The Gerontologist, 58(suppl_1), S88–S102. https://doi.org/10.1093/geront/gnx167
Sykes, D., Tocci, G. C., & Cavanaugh, W. J. (2013). Sound & Vibration 2.0: Design Guidelines for Health Care Facilities (1st ed.). New York, NY: Springer-Verlag.
World Health Organization (WHO). (2018). Ageing and Health. Retrieved from Fact Sheets website: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health
Taking advantage of the collective knowledge and expertise in attendance, this webinar will offer interdisciplinary perspectives to evaluate current cutting edge design solutions, help attendees to develop solutions of their own, and inspire further research with the aspiration to transform the future of the care team station in inpatient behavioral health settings.
This webinar will review two case studies of built behavioral health areas within existing emergency department. We will provide an in-depth look at the materials, products and systems developed to provide safe and durable environments with special attention given to anti- ligature and durability.





 Considering the broad and frequent use of all healthcare options and settings by individuals with dementias (Appendix C), it stands to reason that environmental strategies could be successfully applied across the continuum of care, as well as in private residences, community settings, hospitality hubs, and beyond (Alzheimer’s Association, 2018; Crimmins, 2015; Hebert et al., 2013; Nelson et al., 2019).
Considering the broad and frequent use of all healthcare options and settings by individuals with dementias (Appendix C), it stands to reason that environmental strategies could be successfully applied across the continuum of care, as well as in private residences, community settings, hospitality hubs, and beyond (Alzheimer’s Association, 2018; Crimmins, 2015; Hebert et al., 2013; Nelson et al., 2019).